
Acceptability and Feasibility of a 13-Week Pilot Randomised Controlled Trial Testing the Effects of Incremental Doses of Beetroot Juice in Overweight and Obese Older Adults

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants and Study Design
2.3. Primary and Secondary Outcome Measures
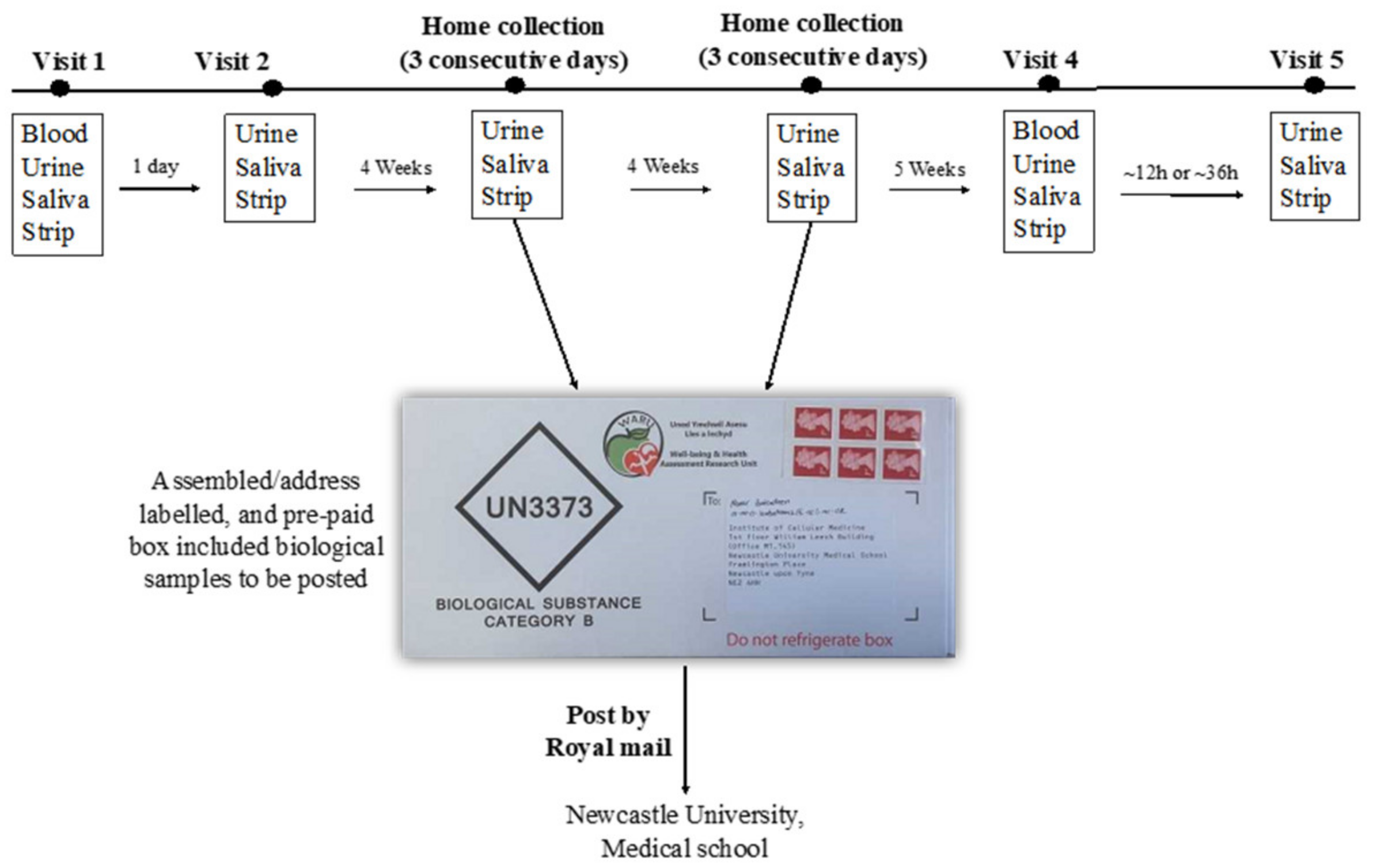
2.4. Data Collection Procedures
2.5. Compliance
2.5.1. Compliance with the Dietary Intervention
2.5.2. Compliance with the Study Protocol
2.6. Recording Food Intake Using Intake24
2.7. Collection and Analysis of Biological Samples
2.8. Acceptability with Intervention and Study Protocol
2.9. Sample Size Calculation
2.10. Data Presentation and Statistical Analysis
3. Results
3.1. Baseline Characteristics
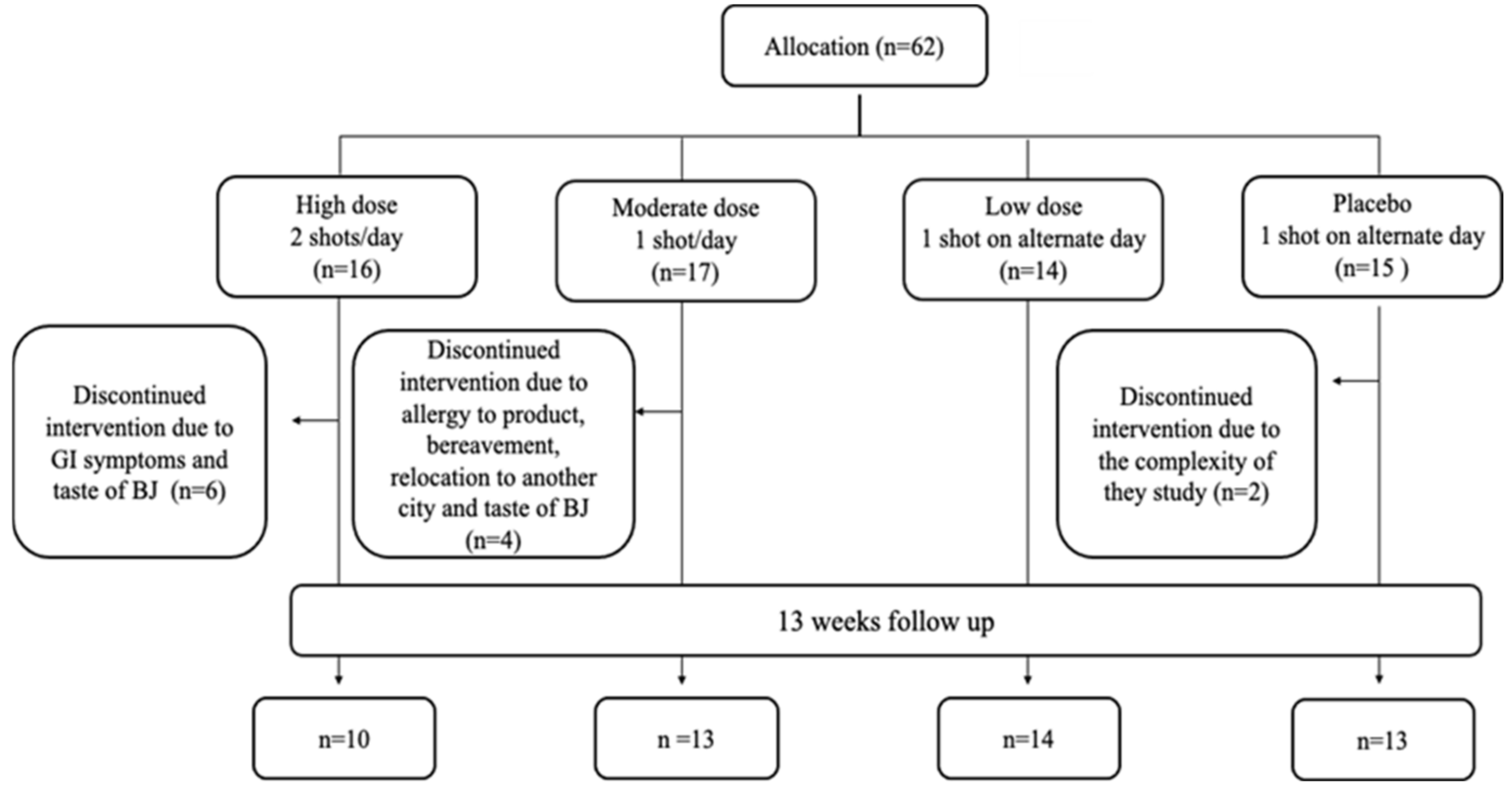
3.2. Recruitment and Retention
3.3. Compliance
3.3.1. Intervention Intake
3.3.2. Sample Collection at Home and Delivery by Post to the Research Centre
3.3.3. Recording Dietary Intake Using Intake24
3.4. Biomarkers of Nitrate Intake
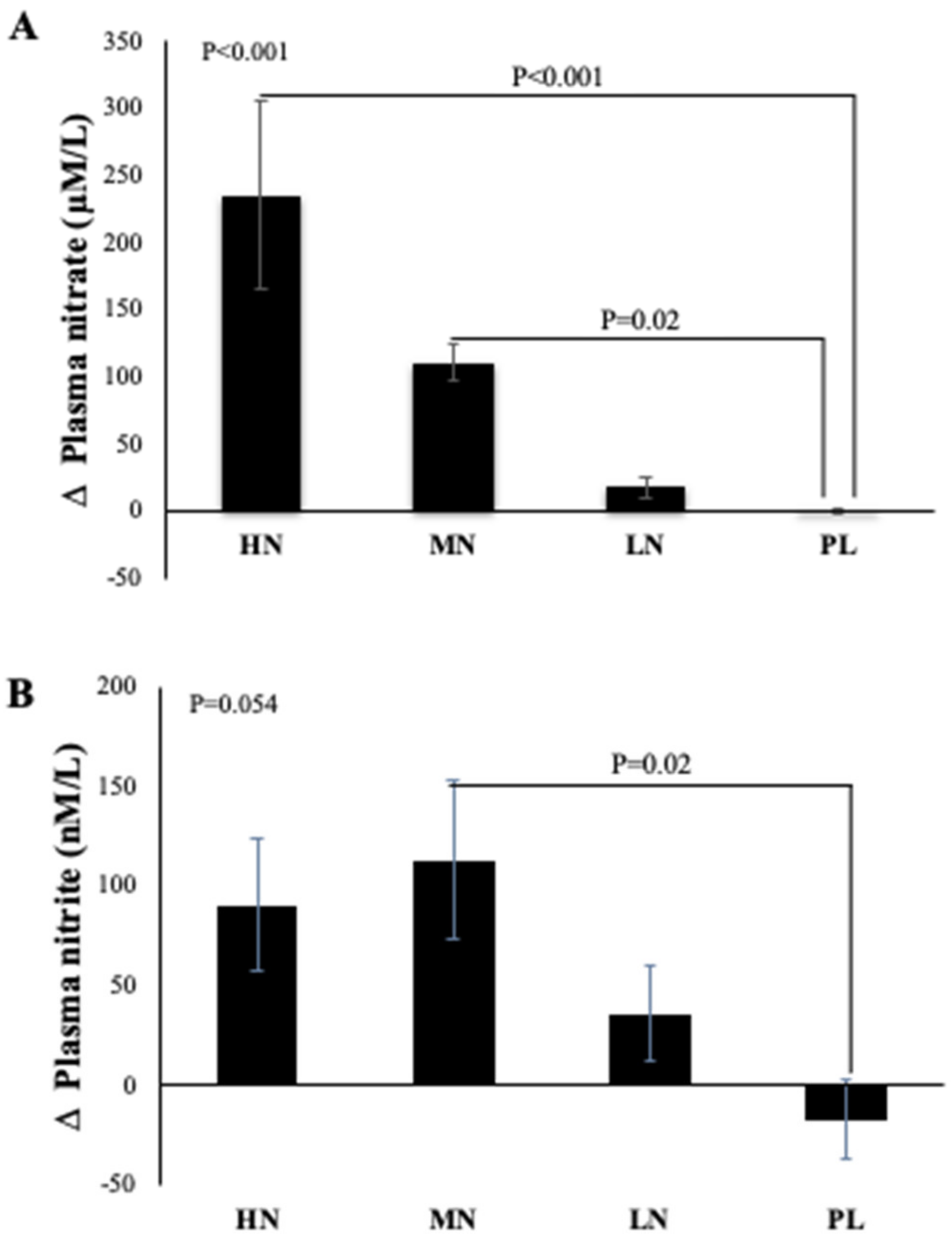
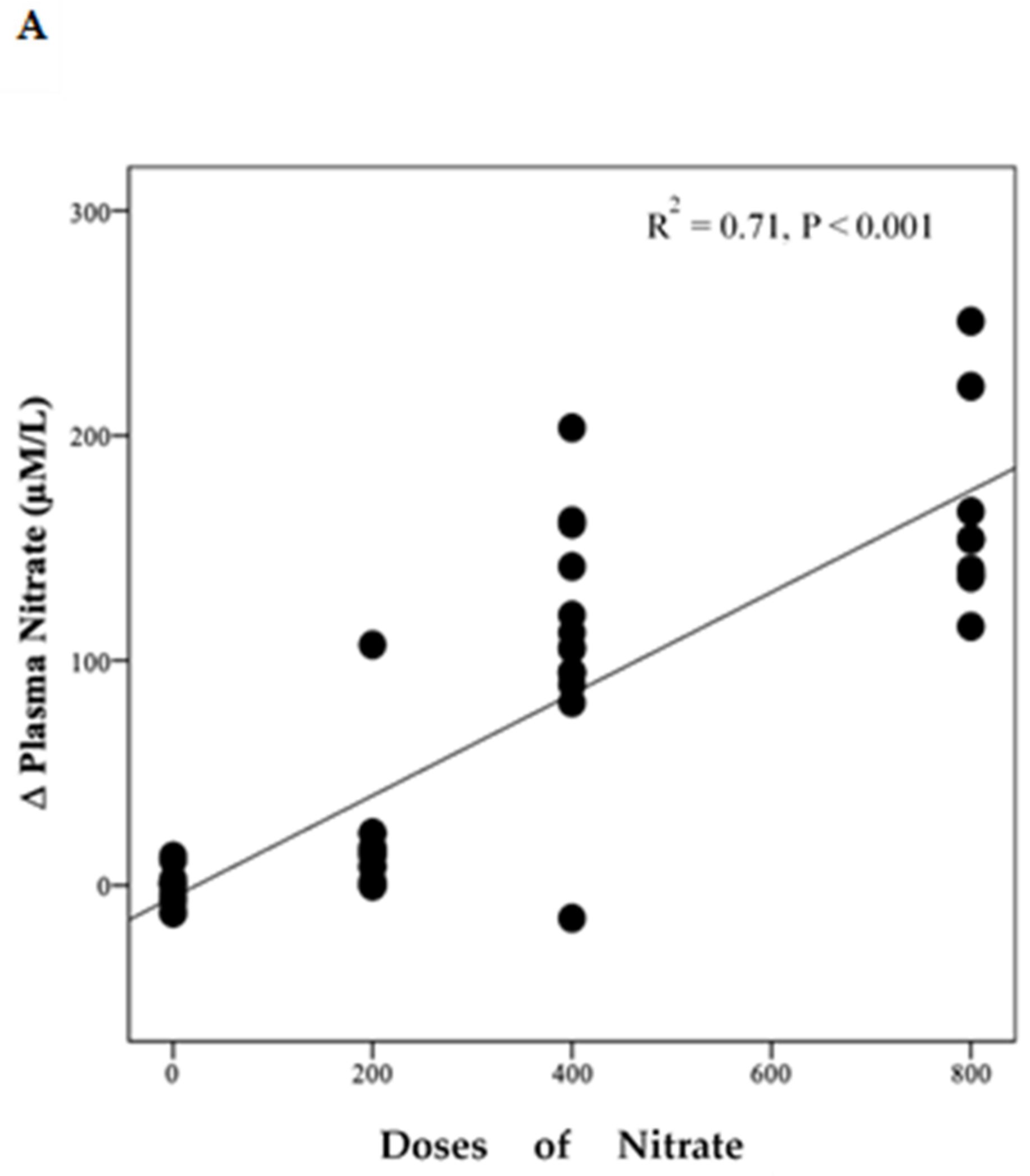
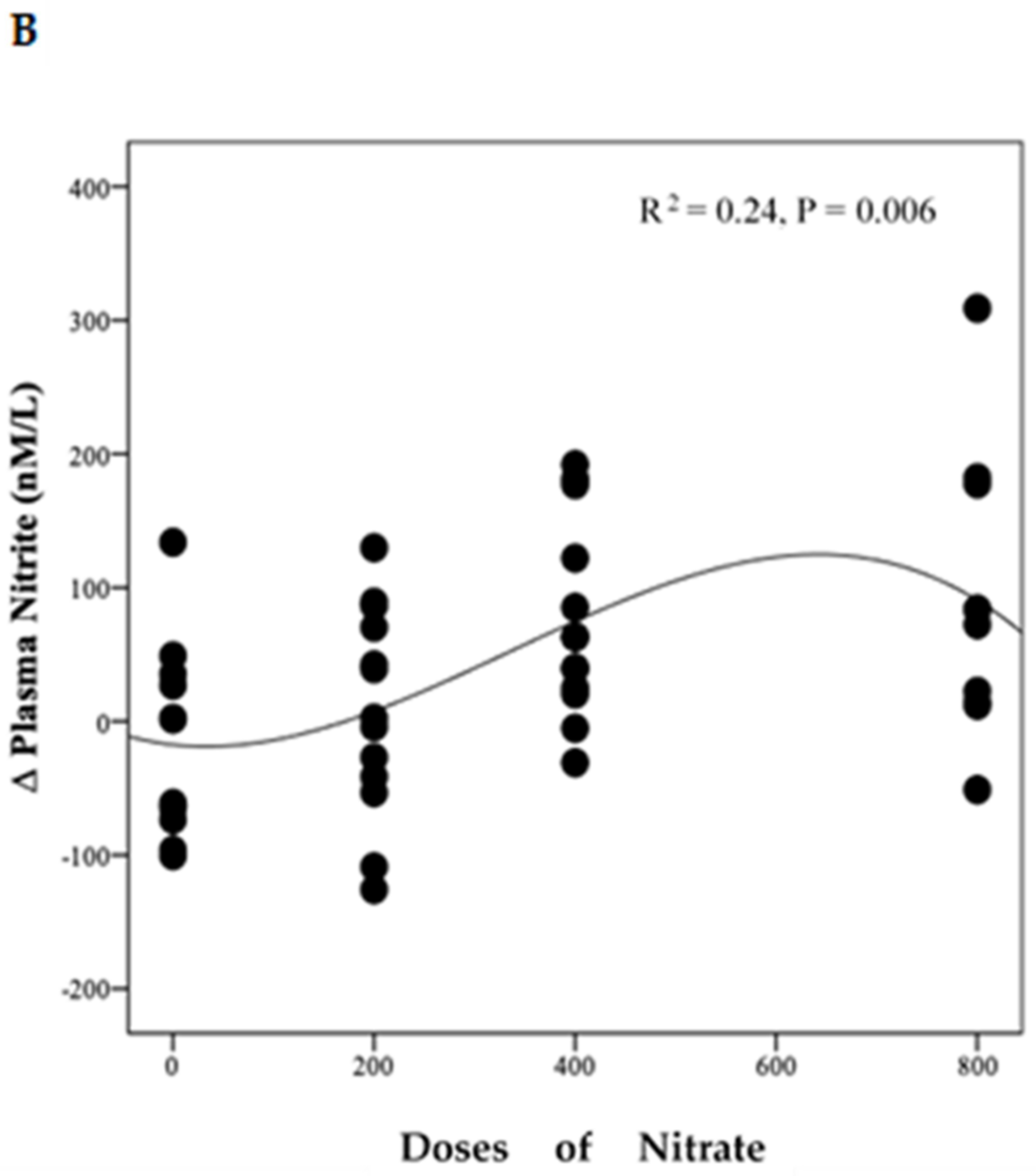
3.4.1. Plasma Nitrate and Nitrite Concentrations
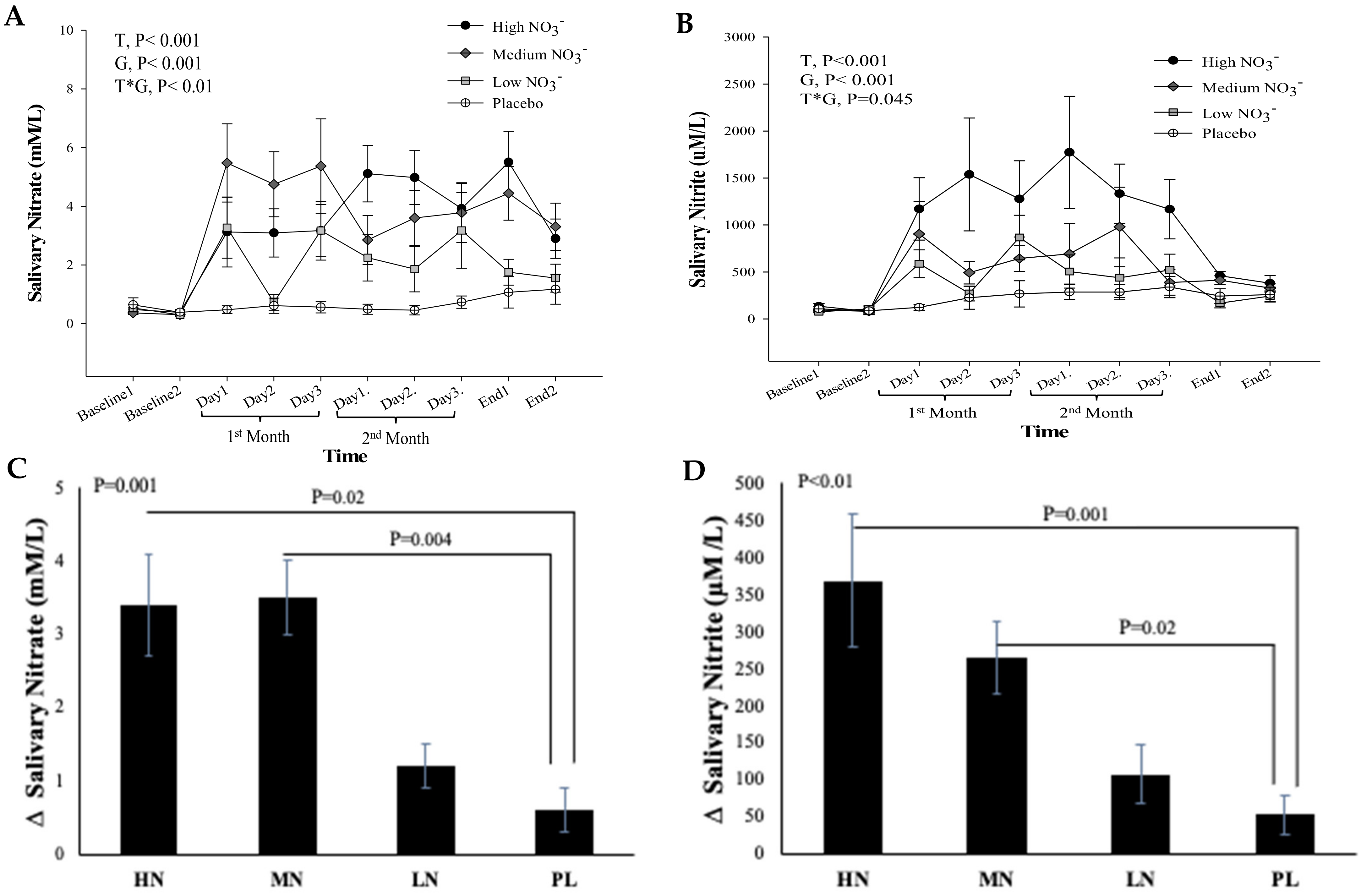
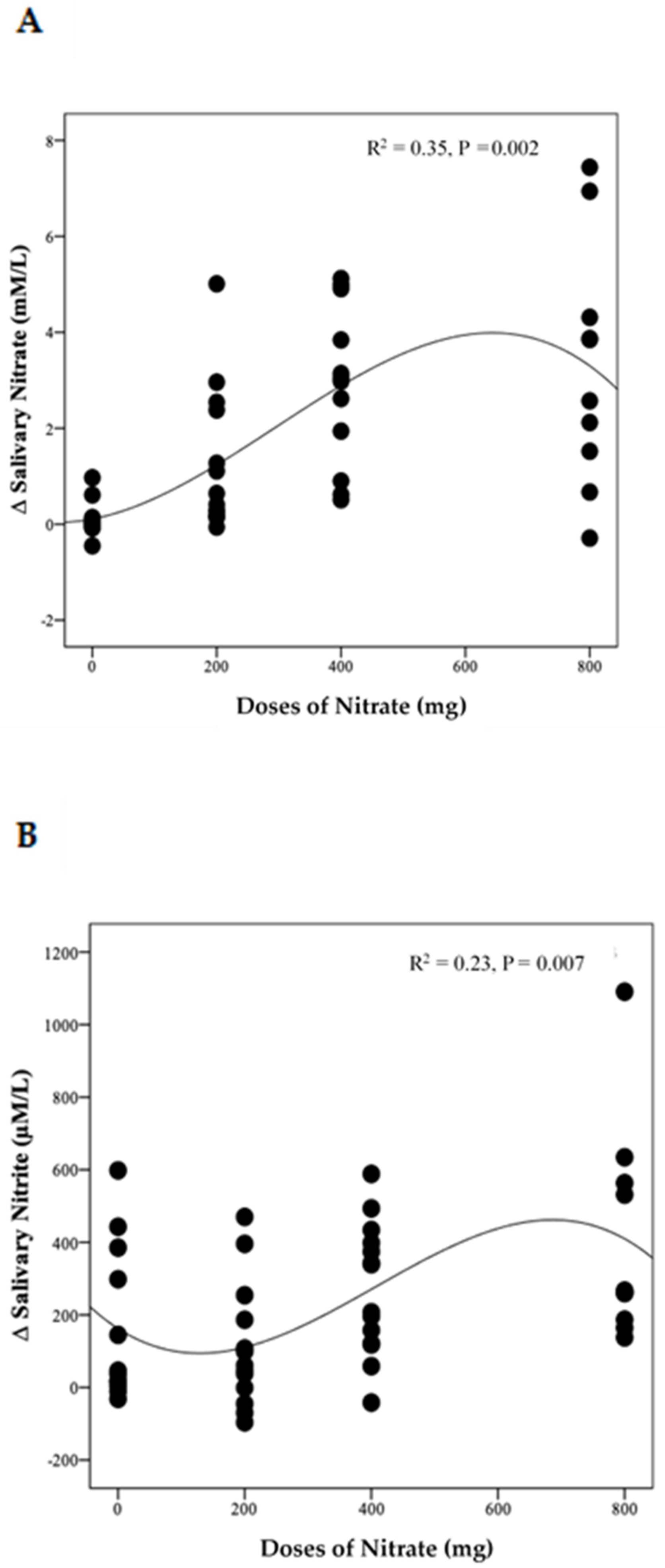
3.4.2. Salivary Nitrate and Nitrite Concentrations
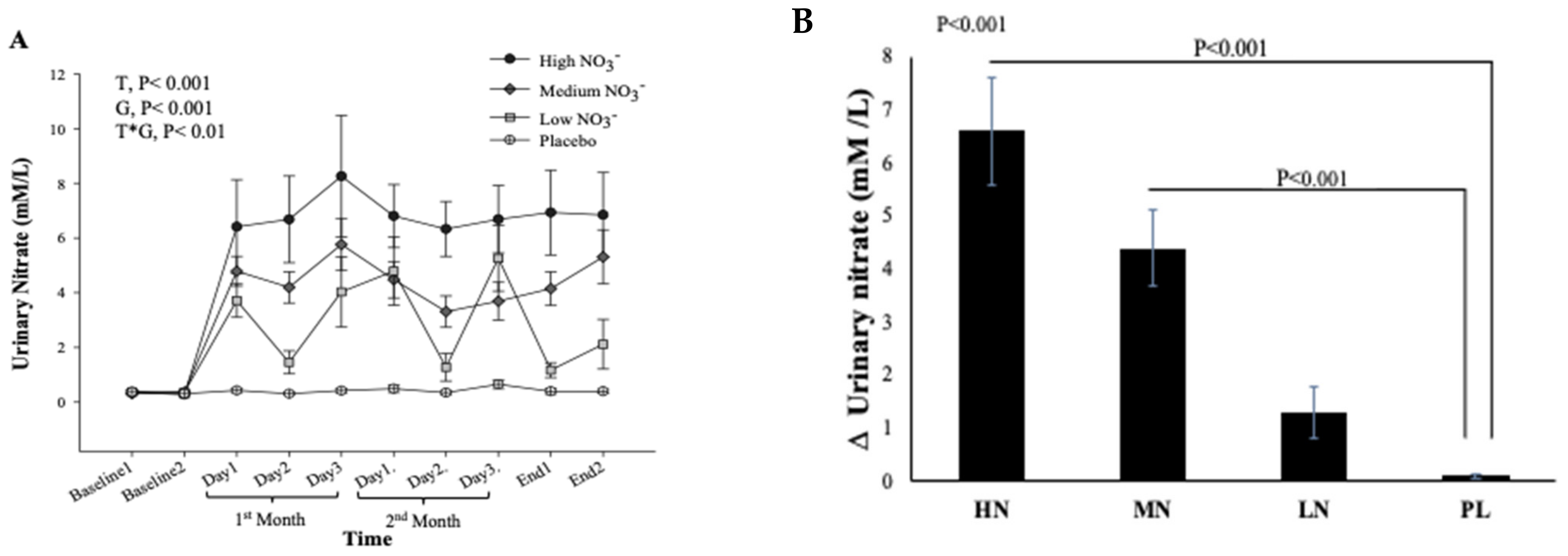
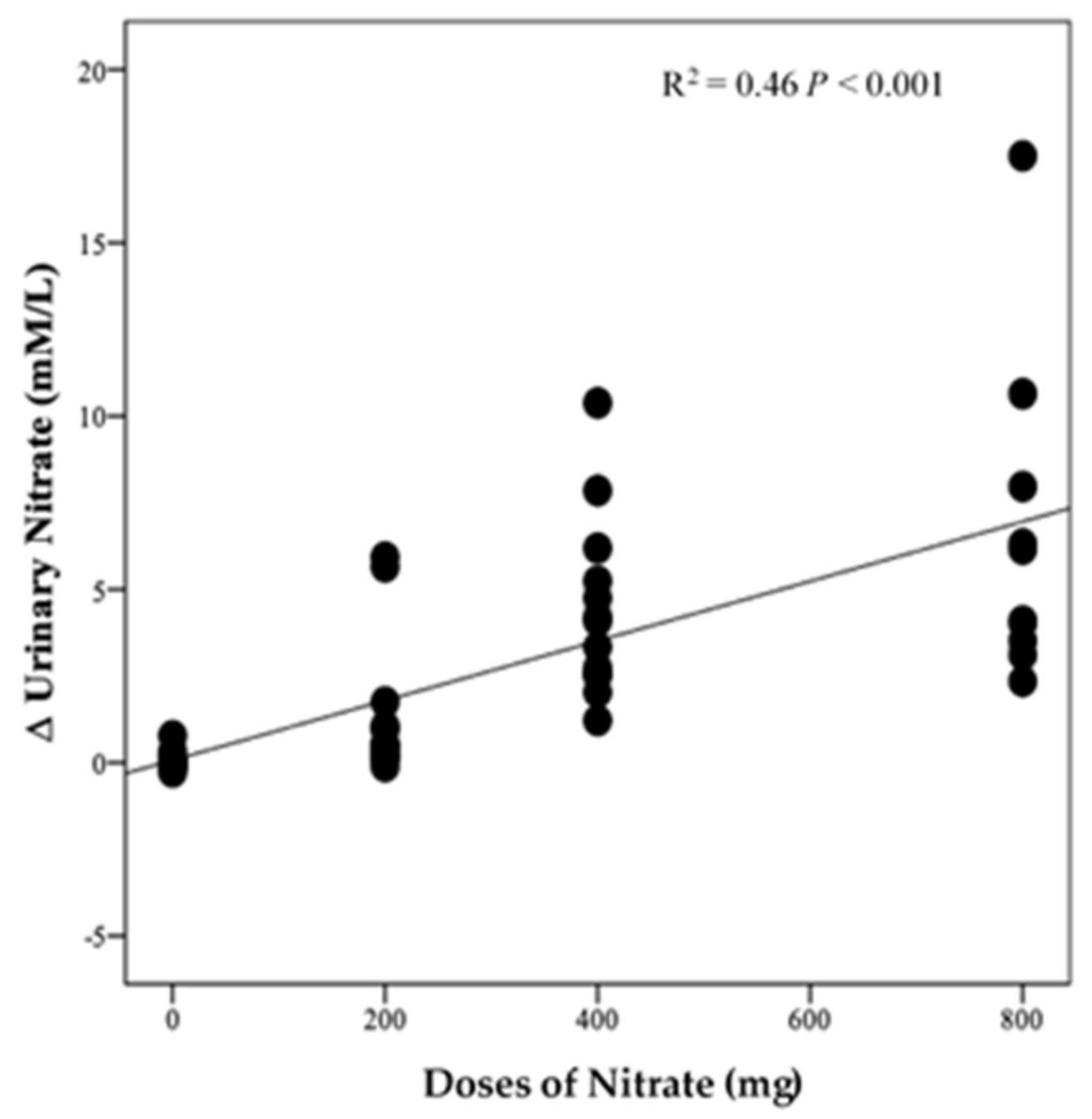
3.4.3. Urinary Nitrate Concentration
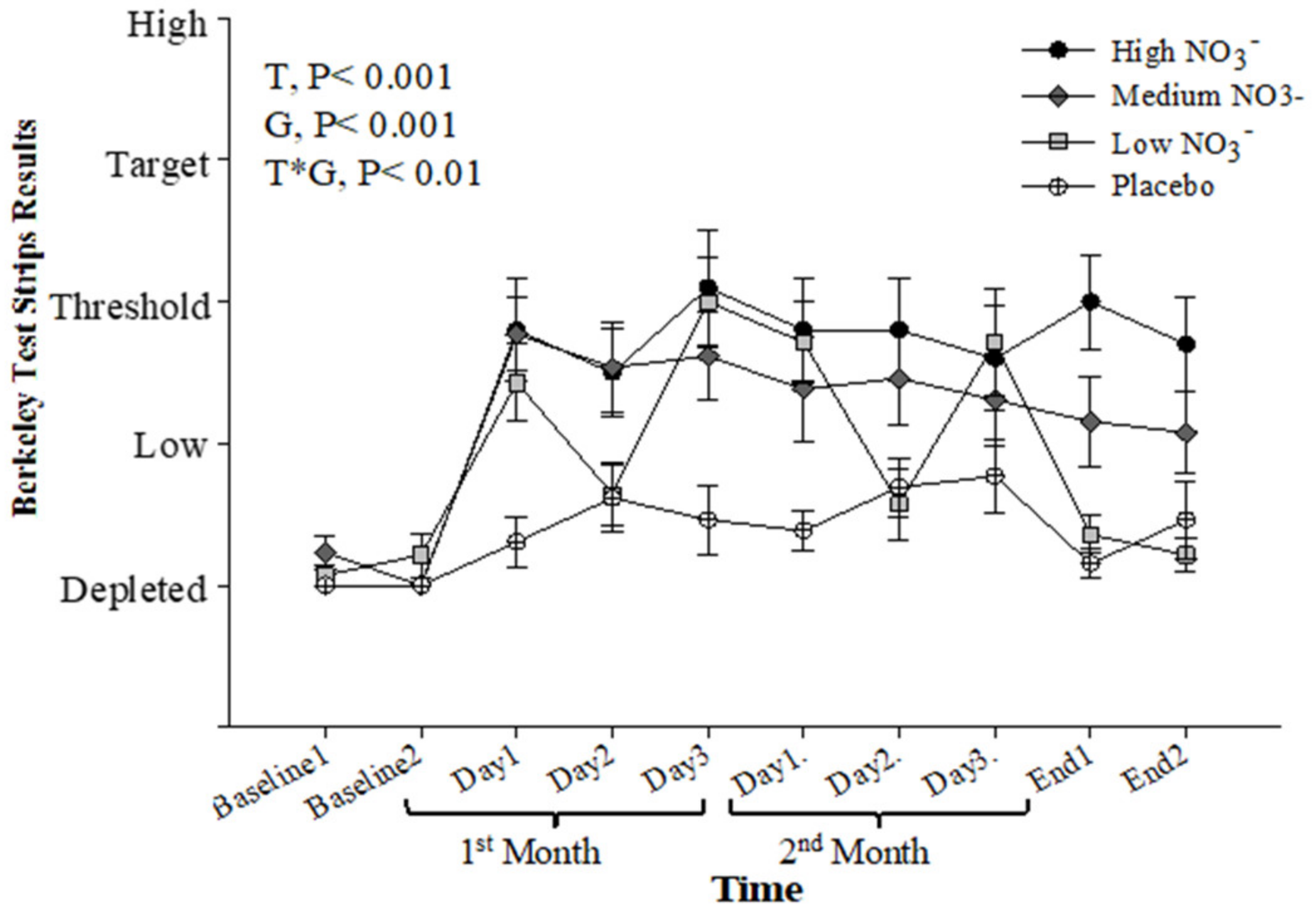
3.4.4. Salivary Nitrite Strips
3.5. The Relationship between the Duration of Postal Delivery Time and the Concentration of NO2− and NO3− Saliva and Urine
3.6. Acceptability of Dietary Intervention and Study Protocol
4. Discussion
4.1. Recruitment and Attrition
4.2. Compliance with Dietary Intervention
4.3. Collection of Biological Samples at Home and Transfer to the Research Centre by Post
4.4. Biomarkers of Nitrate Intake after Prolonged Beetroot Juice (BJ) Consumption
4.4.1. Plasma Nitrate and Nitrite
4.4.2. Salivary Nitrate and Nitrite
4.4.3. Salivary Nitrite Strips
4.4.4. Urinary Nitrate
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Niccoli, T.; Partridge, L. Ageing as a risk factor for disease. Curr. Biol. 2012, 22, R741–R752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storey, A. Living Longer—How our Population Is Changing and Why It Matters; Office for National Statistics: London, UK, 2018.
- Malcomson, F.C.; Mathers, J.C. Nutrition and ageing. In Biochemistry and Cell Biology of Ageing: Part I Biomedical Science; Springer: Berlin/Heidelberg, Germany, 2018; pp. 373–424. [Google Scholar]
- Ridda, I.; Macintyre, C.; Lindley, R.; Tan, T. Difficulties in recruiting older people in clinical trials: An examination of barriers and solutions. Vaccine 2010, 28, 901–906. [Google Scholar] [CrossRef]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical costs of fatal and nonfatal falls in older adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Cherubini, A.; Gasperini, B. How to Increase the Participation of Older Subjects in Research: Good Practices and more Evidence Are Needed! Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Knechel, N.A. The challenges of enrolling older adults into intervention studies. Yale J. Biol. Med. 2013, 86, 41. [Google Scholar]
- Cusack, S.; O’toole, P.W. Challenges and implications for biomedical research and intervention studies in older populations: Insights from the ELDERMET study. Gerontology 2013, 59, 114–121. [Google Scholar] [CrossRef]
- Akmatov, M.K.; Jentsch, L.; Riese, P.; May, M.; Ahmed, M.; Werner, D.; Rosel, A.; Prokein, J.; Bernermann, I.; Klopp, N.; et al. Motivations for (non) participation in population-based health studies among the elderly—Comparison of participants and nonparticipants of a prospective study on influenza vaccination. BMC Med. Res. Methodol. 2017, 17, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crichton, G.E.; Howe, P.R.; Buckley, J.D.; Coates, A.M.; Murphy, K.J.; Bryan, J. Long-term dietary intervention trials: Critical issues and challenges. Trials 2012, 13, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toda, N.; Okamura, T. Obesity impairs vasodilatation and blood flow increase mediated by endothelial nitric oxide: An overview. J. Clin. Pharmacol. 2013, 53, 1228–1239. [Google Scholar] [CrossRef]
- Raubenheimer, K.; Hickey, D.; Leveritt, M.; Fassett, R.; De Zevallos Munoz, J.; Allen, J.D.; Briskey, D.; Parker, T.J.; Kerr, G.; Peake, J.M.; et al. Acute Effects of Nitrate-Rich Beetroot Juice on Blood Pressure, Hemostasis and Vascular Inflammation Markers in Healthy Older Adults: A Randomized, Placebo-Controlled Crossover Study. Nutrients 2017, 9, 1270. [Google Scholar] [CrossRef] [Green Version]
- Jajja, A.; Sutyarjoko, A.; Lara, J.; Rennie, K.; Brandt, K.; Qadir, O.; Seirvo, M. Beetroot supplementation lowers daily systolic blood pressure in older, overweight subjects. Nutr. Res. 2014, 34, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Vanhatalo, A.; Kelly, J.; Winyard, P.G.; Fulford, J.; Jones, A.M. Dietary Nitrate Reduces Blood Pressure and Improves Walking Economy and Cognitive Function in Older People: 910 Board# 226 June 1, 330 PM-500 PM. Med. Sci. Sports Exerc. 2016, 48, 257. [Google Scholar]
- Babateen, A.M.; Rubele, S.; Shannon, O.M.; Okello, E.; Smith, E.; McMahon, N.; O’Brien, G.M.; Wightman, E.; Kennedy, D.; Mathers, J.C.; et al. Protocol and recruitment results from a 13-week randomized controlled trial comparing the effects of different doses of nitrate-rich beetroot juice on cognition, cerebral blood flow and peripheral vascular function in overweight and obese older people. Contemp. Clin. Trials Commun. 2020, 18, 100571. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelun, U.; Yangve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Kapil, V.; Haydar, S.M.; Pearl, V.; Lundberg, J.O.; Weitzberg, E.; Ahluwalia, A. Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free Radic. Biol. Med. 2013, 55, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Foster, E.; Hawkins, A.; Delve, J.; Adamson, A.J. Reducing the cost of dietary assessment: Self-Completed Recall and Analysis of Nutrition for use with children (SCRAN 24). J. Hum. Nutr. Diet. 2014, 27, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Shannon, O.M.; Duckworth, L.; Barlow, M.J.; Woods, D.; Lara, J.; Seirvo, M.; O’Hara, J.P. Dietary nitrate supplementation enhances high-intensity running performance in moderate normobaric hypoxia, independent of aerobic fitness. Nitric Oxide 2016, 59, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Justice, J.N.; Johnson, L.C.; DeVan, A.E.; Cruickshank-Quinn, C.; Reisdroph, N.; Bassett, C.J.; Evans, T.D.; Brooke, F.A.; Bryan, N.; Chonchol, M.B.; et al. Improved motor and cognitive performance with sodium nitrite supplementation is related to small metabolite signatures: A pilot trial in middle-aged and older adults. Aging (Albany N. Y.) 2015, 7, 1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.; Fulford, J.; Vanhatalo, A.; Blackwell, J.R.; French, O.; Bailey, S.J.; Gilchrist, M.; Winyard, P.G.; Jones, A.M. Effects of short-term dietary nitrate supplementation on blood pressure, O2 uptake kinetics, and muscle and cognitive function in older adults. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 304, R73–R83. [Google Scholar] [CrossRef] [Green Version]
- D’El-Rei, J.; Cunha, A.; Trindade, M.; Neves, M.F. Beneficial effects of dietary nitrate on endothelial function and blood pressure levels. Int. J. Hypertens. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Khalifi, S.; Rahimipour, A.; Jeddi, S.; Ghanbari, M.; Kazerouni, F.; Ghasemi, A. Dietary nitrate improves glucose tolerance and lipid profile in an animal model of hyperglycemia. Nitric Oxide 2015, 44, 24–30. [Google Scholar] [CrossRef]
- Presley, T.D.; Morgan, A.R.; Bechtold, E.; Clodfelter, W.; Dove, R.W.; Jennings, J.M.; Kraft, R.A.; King, S.B.; Laurienti, P.J.; Rejeski, W.J.; et al. Acute effect of a high nitrate diet on brain perfusion in older adults. Nitric Oxide 2011, 24, 34–42. [Google Scholar] [CrossRef]
- Allen, J.D.; Giordano, T.; Kevil, C.G. Nitrite and nitric oxide metabolism in peripheral artery disease. Nitric Oxide 2012, 26, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudha, M.R.; Ahire, J.J.; Tripathi, A.; Nanal, S. Effect of multi-strain probiotic (UB0316) in weight management in overweight/obese adults: A 12-week double blind, randomised, placebo-controlled study. Benef. Microbes 2019, 10, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Jonvik, K.L.; Willem Van Dijk, J.; Senden, J.M.; van Loon, L.J.; Verdijk, L.B. The effect of beetroot juice supplementation on dynamic apnea and intermittent sprint performance in elite female water polo players. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 468–473. [Google Scholar] [CrossRef] [Green Version]
- Jonvik, K.L.; Nyakayiru, J.; Van Dijk, J.W.; Maase, K.; Ballak, S.B.; Senden, J.M.; Van Loon, L.J.; Verdijk, L.B. Repeated-sprint performance and plasma responses following beetroot juice supplementation do not differ between recreational, competitive and elite sprint athletes. Eur. J. Sport Sci. 2018, 18, 524–533. [Google Scholar] [CrossRef] [PubMed]
- James, P.E.; Willis, G.; Allen, J.D.; Winyard, P.G.; Jones, A.M. Nitrate pharmacokinetics: Taking note of the difference. Nitric Oxide 2015, 48, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Desroches, S.; Lapinte, A.; Ratte, S.; Gravel, K.; Legare, F.; Turcotte, S. Interventions to enhance adherence to dietary advice for preventing and managing chronic diseases in adults. Cochrane Database Syst. Rev. 2013, 28, CD008722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blekkenhorst, L.C.; Lewis, J.; Prince, R.L.; Devine, A.; Bondonno, N.; Bondonno, C.; Wood, L.; Puddey, L.B.; Ward, N.C.; Croft, K.D.; et al. Nitrate-rich vegetables do not lower blood pressure in individuals with mildly elevated blood pressure: A 4-wk randomized controlled crossover trial. Am. J. Clin. Nutr. 2018, 107, 894–908. [Google Scholar] [CrossRef]
- Rockett, J.C.; Buck, G.M.; Lynch, C.D.; Perreault, S.D. The value of home-based collection of biospecimens in reproductive epidemiology. Environ. Health Perspect. 2004, 112, 94–104. [Google Scholar] [CrossRef]
- Cox, K.J.; Stanford, J.B.; Blackburn, B.E.; Porucznik, C.A. Compliance with daily, home-based collection of urinary biospecimens in a prospective, preconception cohort. Environ. Epidemiol. (Phila. Pa.) 2019, 3, e050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Hu, L.; Feng, X.; Wang, S. Nitrate and nitrite in health and disease. Aging Dis. 2018, 9, 938. [Google Scholar] [CrossRef] [Green Version]
- Bondonno, C.; Liu, A.H.; Croft, K.D.; Ward, N.C.; Puddey, I.B.; Woodman, R.J.; Hodgson, J.M. Short-term effects of a high nitrate diet on nitrate metabolism in healthy individuals. Nutrients 2015, 7, 1906–1915. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, J.O.; Weitzberg, E. NO-synthase independent NO generation in mammals. Biochem. Biophys. Res. Commun. 2010, 396, 39–45. [Google Scholar] [CrossRef]
- Doel, J.J.; Benjamin, N.; Hector, M.P.; Rogers, M.; Allaker, R.P. Evaluation of bacterial nitrate reduction in the human oral cavity. Eur. J. Oral Sci. 2005, 113, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Burleigh, M.; Liddle, L.; Muggeridge, D.J.; Monaghan, C.; Sculthorpe, N.; Butcher, J.; Henriquez, F.; Easton, C. Dietary nitrate supplementation alters the oral microbiome but does not improve the vascular responses to an acute nitrate dose. Nitric Oxide Biol. Chem. 2019, 89, 54–63. [Google Scholar] [CrossRef]
- Vanhatalo, A.; Blackwell, J.R.; L’Heureux, J.E.; William, D.W.; Smith, A.; Van der Giezen, M.; Winyard, P.G.; Jones, A.M. Nitrate-responsive oral microbiome modulates nitric oxide homeostasis and blood pressure in humans. Free Radic. Biol. Med. 2018, 124, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Thompson, I.; Carter, P.; Whiteley, A.; Bailey, M.; Leifert, C.; Killham, K. Salivary nitrate—An ecological factor in reducing oral acidity. Oral Microbiol. Immunol. 2007, 22, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hohensinn, B.; Haselgrubler, R.; Muller, U.; Stanlbauer, V.; Lanzerstorfer, P.; Lirk, G.; Hoglinger, O.; Weghuber, J. Sustaining elevated levels of nitrite in the oral cavity through consumption of nitrate-rich beetroot juice in young healthy adults reduces salivary pH. Nitric Oxide 2016, 60, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bojić, D.V.; Bojić, A.L.; Perović, J.M. The effects of dietary nitrate, pH and temperature on nitrate reduction in the human oral cavity. Facta Univ. Ser. Phys. Chem. Technol. 2004, 3, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Babateen, A.M.; Shannon, O.M.; Mathers, J.C.; Siervo, M. Validity and reliability of test strips for the measurement of salivary nitrite concentration with and without the use of mouthwash in healthy adults. Nitric Oxide 2019, 91, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D.A.; Schultz, D.S.; Deen, W.M.; Young, V.R.; Tennenbaum, S.R. Metabolic fate of an oral dose of 15N-labeled nitrate in humans: Effect of diet supplementation with ascorbic acid. Cancer Res. 1983, 43, 1921–1925. [Google Scholar]
- Schultz, D.S.; Deen, W.M.; Karel, S.F.; Wagner, D.A.; Tennenbaum, S.R. Pharmacokinetics of nitrate in humans: Role of gastrointestinal absorption and metabolism. Carcinogenesis 1985, 6, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Berends, J.E.; Van den Berg, L.M.; Guggeism, M.A.; Henckens, N.F.; Hossein, I.J.; deJoode, M.E.; Zamani, H.; van Pelt, K.A.; Beelen, N.A.; Kuhnle, G.; et al. Consumption of Nitrate-Rich Beetroot Juice with or without Vitamin C Supplementation Increases the Excretion of Urinary Nitrate, Nitrite, and N-nitroso Compounds in Humans. Int. J. Mol. Sci. 2019, 20, 2277. [Google Scholar] [CrossRef] [Green Version]
- Leach, S.; Packer, P.; Hill, M. Salivary and Urinary Nitrate as Measures of Nitrate Intake; Portland Press Limited: Biochem Soc Tranc: London, UK, 1987. [Google Scholar]
- Bartholomew, B.; Hill, M. The pharmacology of dietary nitrate and the origin of urinary nitrate. Food Chem. Toxicol. 1984, 22, 789–795. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | HN | MN | LN | PL | p-Value | |
|---|---|---|---|---|---|---|
| Characteristics | ||||||
| Number | 62 | 16 | 17 | 14 | 15 | - |
| Gender, M/F | 24/38 | 10/6 | 12/5 | 4/10 | 5/10 | 0.16 |
| Age (years) | 66.3 ± 3.7 | 64.7 ± 3.5 | 66.7 ± 4.2 | 67.3 ± 2.7 | 65.7 ± 3.9 | 0.16 |
| Education (years) | 15.3 ± 3.0 | 16.0 ± 3 | 15.7 ± 2.6 | 15.0 ± 3.1 | 14.6 ± 3.1 | 0.73 |
| Body weight (kg) | 84.9 ± 12.6 | 90.9 ± 13.4 | 84.6 ± 10.5 | 80.1 ± 12.5 | 83.9 ± 12.6 | 0.15 |
| BMI (kg/m2) | 30.3 ± 3.7 | 30.5 ± 3.6 | 30.5 ± 3.2 | 29.9 ± 3.4 | 30.3 ± 4.8 | 0.99 |
| WC (cm) | 102.4 ± 9.2 | 104.5 ± 10.3 | 100.6 ± 9.6 | 102.1 ± 8.9 | 102.6 ± 8.2 | 0.59 |
| FM (kg) | 32.4 ± 8.7 | 32.1 ± 8.7 | 34.5 ± 9.0 | 31.3 ± 7.2 | 31.5 ± 10.0 | 0.90 |
| FM (%) | 37.8 ± 7.8 | 35.2 ± 8.2 | 39.2 ± 7.8 | 39.3 ± 6.6 | 37.1 ± 8.1 | 0.41 |
| TBW (kg) | 38.6 ± 6.3 | 41.3 ± 7.4 | 38.6 ± 4.5 | 35.6 ± 6.3 | 38.8 ± 5.9 | 0.18 |
| SBP (mm Hg) | 135.1 ± 14.7 | 130.8 ± 12.0 | 136.1 ± 10.4 | 139.5 ± 13.2 | 134.1 ± 12.9 | 0.46 |
| DBP (mm Hg) | 76.9 ± 9.4 | 75.8 ± 9.7 | 77.3 ± 9.1 | 77.8 ± 8.1 | 76.9 ± 11.2 | 0.96 |
| PA (METs/week) | 3667 ± 5604 | 2741 ± 1522 | 3257 ± 1845 | 2262 ± 1933 | 6280 ± 10512 | 0.20 |
| Medication use | ||||||
| Antihypertensive | 6 (9.8%) | 1 (6%) | 1 (6%) | 1 (7%) | 3 (20%) | - |
| Hormonal therapy Thyroxin Testosterone | 9 (14.5%) 1 (1.6%) | 3 (19%) 1 | 1 (6%) 0 | 4 (29%) 0 | 1 (7%) 0 | - - |
| Antihistamine | 1 (1.6%) | 0 | 0 | 1 (7%) | 0 | - |
| Lipid lowering agents | 10 (16%) | 5 (31%) | 2 (12%) | 1 (7%) | 2 (13%) | - |
| Vitamin D | 3 (3%) | 1 (6%) | 2 (12%) | 0 | 0 | - |
| Aspirin | 1 (1.6%) | 0 | 0 | 0 | 1 (7%) | - |
| Corticosteroid inhalers | 2 (3%) | 0 | 1 (6%) | 0 | 1 (7%) | - |
| No therapy | 35 (56%) | 10 (63%) | 9 (53%) | 7 (50%) | 9 (60%) | - |
| Reasons | N (%) | Specific Reasons Provided by Participants |
|---|---|---|
| Uncomfortable bowel movement | 3 (25) | “The number of times I spent going to the toilet increased, I go to the toilet up to eight times a day, it is obvious that something in the supplement has a certain effect on me” “I drank the beetroot juice (BJ), within 15 min I had to rush to the lavatory with diarrhoea”. “I need to give up, BJ seems to be giving me extremely loose bowels and I have had to stop taking it” |
| Taste and smell of BJ | 3 (25) | “The smell, taste and texture are all extremely unpleasant, leaving me with a feeling of nausea for a long time after taking the BJ (Sometimes hours)”. “I am so sorry I have to pull out, because of the horrible taste of BJ, I was cheating: can’t drink all of the bottle, don’t want to spoil your study” “There is a fundamental problem in that I can’t tolerate the juice. I hate the juice; the consistency makes me feel sick and it is way too sweet. Much as I love beetroot, I cannot drink this”. |
| Moving out of the area | 1 (8) | “I regret to say due to an enormous amount of travelling I have had to endure recently, I will have to drop out from your research scheme” |
| Complicated study | 2 (16) | “Sorry, but I find it all a chore, with travelling in and out of town. Sorry I would like to exit from trial” |
| Teeth problems | 1 (8) | “Unfortunately, I do think I will need to stop the study. too much sugar in the juices which are spoiling my teeth, I often have headaches after I drink them” |
| Bereavement family | 1 (8) | - |
| Mouthwash use | 1 (8) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babateen, A.M.; Shannon, O.M.; O’Brien, G.M.; Okello, E.; Khan, A.A.; Rubele, S.; Wightman, E.; Smith, E.; McMahon, N.; Olgacer, D.; et al. Acceptability and Feasibility of a 13-Week Pilot Randomised Controlled Trial Testing the Effects of Incremental Doses of Beetroot Juice in Overweight and Obese Older Adults. Nutrients 2021, 13, 769. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030769
Babateen AM, Shannon OM, O’Brien GM, Okello E, Khan AA, Rubele S, Wightman E, Smith E, McMahon N, Olgacer D, et al. Acceptability and Feasibility of a 13-Week Pilot Randomised Controlled Trial Testing the Effects of Incremental Doses of Beetroot Juice in Overweight and Obese Older Adults. Nutrients. 2021; 13(3):769. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030769
Chicago/Turabian StyleBabateen, Abrar M., Oliver M. Shannon, Gerard M. O’Brien, Edward Okello, Anmar A. Khan, Sofia Rubele, Emma Wightman, Ellen Smith, Nicholas McMahon, Dilara Olgacer, and et al. 2021. "Acceptability and Feasibility of a 13-Week Pilot Randomised Controlled Trial Testing the Effects of Incremental Doses of Beetroot Juice in Overweight and Obese Older Adults" Nutrients 13, no. 3: 769. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030769