
Initial Evidence of Variation by Ethnicity in the Relationship between Vitamin C Status and Mental States in Young Adults


 and
and
Abstract
:1. Introduction
2. Materials and Methods
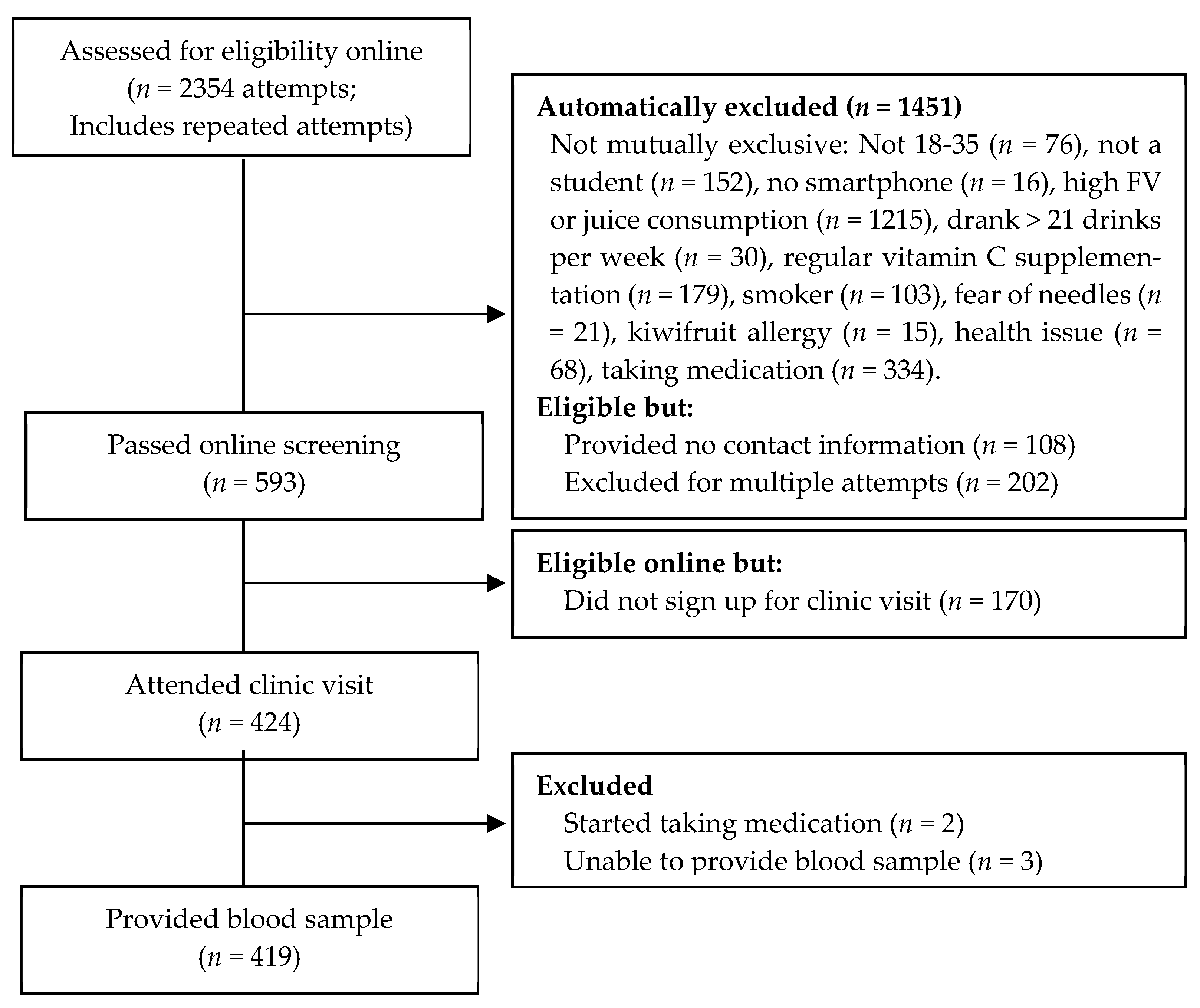
2.1. Participants and Procedure
2.2. Measures
2.2.1. Vitamin C Analysis
2.2.2. Demographics
2.2.3. Mood
2.2.4. Vitality
2.2.5. Stress
2.3. Analysis
3. Results
3.1. Descriptive Statistics
3.2. Relationship between Vitamin C and Mood, Vitality, and Stress
3.2.1. Overall Sample
3.2.2. Moderation by Gender
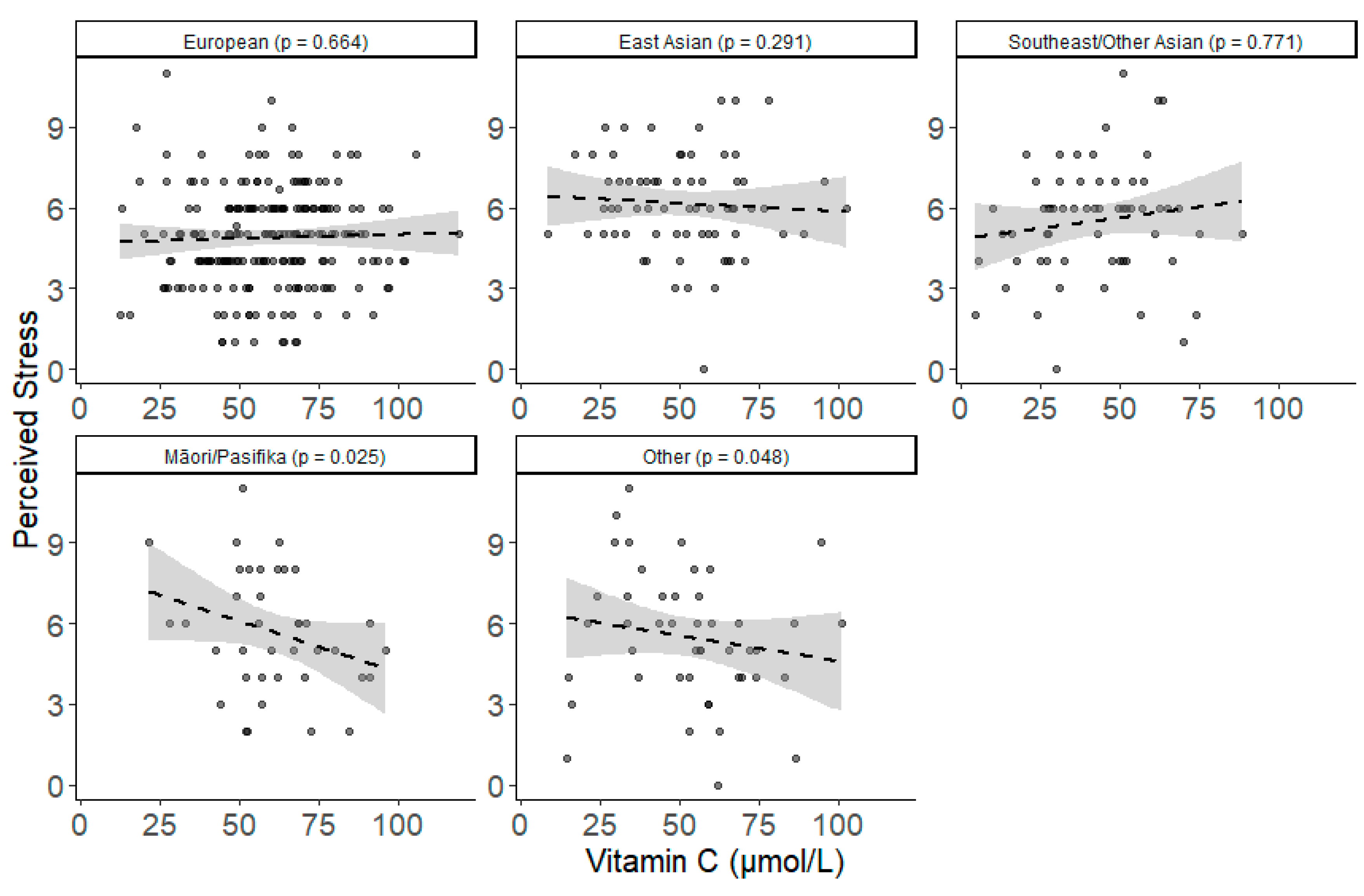
3.2.3. Moderation by Ethnicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carr, A.C.; Bozonet, S.M.; Pullar, J.M.; Vissers, M.C. Mood improvement in young adult males following supplementation with gold kiwifruit, a high-vitamin C food. J. Nutr. Sci. 2013, 2, e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conner, T.S.; Brookie, K.L.; Carr, A.C.; Mainvil, L.A.; Vissers, M.C. Let them eat fruit! The effect of fruit and vegetable consumption on psychological well-being in young adults: A randomized controlled trial. PLoS ONE 2017, 12, e0171206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchflower, D.G.; Oswald, A.J.; Stewart-Brown, S. Is psychological well-being linked to the consumption of fruit and vegetables? Soc. Indic. Res. 2013, 114, 785–801. [Google Scholar] [CrossRef] [Green Version]
- McMartin, S.E.; Jacka, F.N.; Colman, I. The association between fruit and vegetable consumption and mental health disorders: Evidence from five waves of a national survey of Canadians. Prev. Med. 2013, 56, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Mujcic, R.; Oswald, A.J. Evolution of well-being and happiness after increases in consumption of fruit and vegetables. Am. J. Public Health. 2016, 106, 1504–1510. [Google Scholar] [CrossRef]
- White, B.A.; Horwath, C.C.; Conner, T.S. Many apples a day keep the blues away-daily experiences of negative and positive affect and food consumption in young adults. Br. J. Health Psychol. 2013, 18, 782–798. [Google Scholar] [CrossRef]
- Pullar, J.M.; Carr, A.C.; Bozonet, S.M.; Vissers, M. High vitamin C status is associated with elevated mood in male tertiary students. Antioxidants 2018, 7, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Liu, X.J.; Robitaille, L.; Eintracht, S.; MacNamara, E.; Hoffer, L.J. Effects of vitamin C and vitamin D administration on mood and distress in acutely hospitalized patients. Am. J. Clin. Nutr. 2013, 98, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Conner, T.S.; Fletcher, B.D.; Pullar, J.M.; Spencer, E.; Mainvil, L.A.; Vissers, M.C.M. KiwiC for Vitality: Results of a randomized placebo-controlled trial testing the effects of kiwifruit or vitamin C tablets on vitality in adults with low vitamin C levels. Nutrients 2020, 12, 2898. [Google Scholar] [CrossRef]
- Harrison, F.E.; May, J.M. Vitamin C function in the brain: Vital role of the ascorbate transporter SVCT2. Free Radic. Biol. Med. 2009, 46, 719–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikimi, M.; Fukuyama, R.; Minoshima, S.; Shimizu, N.; Yagi, K. Cloning and chromosomal mapping of the human nonfunctional gene for L-gulono-gamma-lactone oxidase, the enzyme for L-ascorbic acid biosynthesis missing in man. J. Biol. Chem. 1994, 269, 13685–13688. [Google Scholar] [CrossRef]
- Agarwal, A.; Shaharyar, A.; Kumar, A.; Bhat, M.S.; Mishra, M. Scurvy in pediatric age group-A disease often forgotten? J. Clin. Orthop. Trauma. 2015, 6, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; Frei, B. Toward a new recommended dietary allowance for vitamin C based on antioxidant and health effects in humans. Am. Soc. Clin. Nutr. 1999, 69, 1086–1107. [Google Scholar] [CrossRef] [Green Version]
- Kinsman, R.A.; Hood, J. Some behavioral effects of ascorbic acid deficiency. Am. J. Clin. Nutr. 1971, 24, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Léger, D. Scurvey. Can. Fam. Physician 2008, 54, 1403–1406. [Google Scholar] [PubMed]
- Lykkesfeldt, J.; Poulsen, H.E. Is vitamin C supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2010, 103, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Vissers, M. Good nutrition matters: Hypovitaminosis C associated with depressed mood and poor wound healing. N. Z. Med. J. 2012, 125, 107–109. [Google Scholar]
- Carr, A.; Vissers, M.; Cook, J. Parenteral vitamin C relieves chronic fatigue and pain in a patient presenting with rheumatoid arthritis and mononeuritis multiplex secondary to CNS vasculitis. Case Rep. Clin Path. 2015, 2, 57–61. [Google Scholar]
- Carr, A.C.; Vissers, M.; Cook, J. Relief from cancer chemotherapy side effects with pharmacologic vitamin C. N. Z. Med. J. 2014, 127, 66–70. [Google Scholar] [PubMed]
- Carr, A.C.; Vissers, M.; Cook, J.S. The effect of intravenous vitamin C on cancer-and chemotherapy-related fatigue and quality of life. Front. Oncol. 2014, 4, 283. [Google Scholar] [CrossRef] [Green Version]
- Gariballa, S. Poor vitamin C status is associated with increased depression symptoms following acute illness in older people. Int. J. Vitam Nutr Res. 2014, 84, 12–17. [Google Scholar] [CrossRef]
- Zhang, M.; Robitaille, L.; Eintracht, S.; Hoffer, L.J. Vitamin C provision improves mood in acutely hospitalized patients. Nutrients 2011, 27, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Cheraskin, E.; Ringsdorf, W.M.J.; Medford, F.H. Daily vitamin C consumption and fatigability. J. Am. Geriatr. Soc. 1976, 24, 136–137. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, I.; de Souza, V.; Motta, V.; Da-Silva, S. Effects of oral vitamin C supplementation on anxiety in students: A doubleblind, randomized, placebo-controlled trial. Pak. J. Biol. Sci. 2015, 18, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Vilsaint, C.L.; NeMoyer, A.; Fillbrunn, M.; Sadikova, E.; Kessler, R.C.; Sampson, N.A.; Alvarez, K.; Green, J.G.; McLaughlin, K.A.; Chen, R. Racial/ethnic differences in 12-month prevalence and persistence of mood, anxiety, and substance use disorders: Variation by nativity and socioeconomic status. Compr. Psychiatry 2019, 89, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Duck, I.M.; Sibley, C.G. Ethnic inequality in diagnosis with depression and anxiety disorders. N. Z. Med. J. 2017, 130, 10–20. [Google Scholar] [PubMed]
- Fain, O.; Pariés, J.; Jacquart Bt Le Moël, G.; Kettaneh, A.; Stirnemann, J.; Héron, C.; Sitbon, M.; Taleb, C.; Letellier, E. Hypovitaminosis C in hospitalized patients. Eur. J. Intern. Med. 2003, 14, 419–425. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Christen, S.; Wallock, L.M.; Chang, H.H.; Jacob, R.A.; Ames, B.N. Ascorbate is depleted by smoking and repleted by moderate supplementation: A study in male smokers and nonsmokers with matched dietary antioxidant intakes. Am. J. Clin. Nutr. 2000, 71, 530–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, J.J.; Ellis, S.L.; McVeigh, K.L.; Levine, R.E.; Calles-Escandon, J. Reduced mononuclear leukocyte ascorbic acid content in adults with insulin-dependent diabetes mellitus consuming adequate dietary vitamin C. Metabolism 1991, 40, 146–149. [Google Scholar] [CrossRef]
- Chen, H.; Karne, R.J.; Hall, G.; Campia, U.; Panza, J.A.; Cannon, R.O., III; Wang, Y.; Katz, A.; Levine, M.; Quon, M.J. High-dose oral vitamin C partially replenishes vitamin C levels in patients with Type 2 diabetes and low vitamin C levels but does not improve endothelial dysfunction or insulin resistance. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H137–H145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pullar, J.M.; Bayer, S.; Carr, A.C. Appropriate handling, processing and analysis of blood samples is essential to avoid oxidation of vitamin C to dehydroascorbic acid. Antioxidants 2018, 7, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griskevicius, V.; Delton, A.W.; Robertson, T.E.; Tybur, J.M. Environmental contingency in life history strategies: The influence of mortality and socioeconomic status on reproductive timing. J. Personal. Soc. Psychol. 2011, 100, 241–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heuchert, J.; McNair, D. POMS 2; Multi-Health Systems Incorporated: North Tonawanda, NY, USA, 2012. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. Perceived stress scale. Meas. Stress Guide Health Soc. Sci. 1994, 10, 1–2. [Google Scholar]
- Schleicher, R.L.; Carroll, M.D.; Ford, E.S.; Lacher, D.A. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003–2004 National Health and Nutrition Examination Survey (NHANES). Am. J. Clin. Nutr. 2009, 90, 1252–1263. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.M.; Iqbal, M.P. Deficiency of vitamin C in South Asia. Pak. J. Med Sci. 2006, 22, 347. [Google Scholar]
- Ness, A.R.; Cappuccio, F.P.; Atkinson, R.W.; Khaw, K.-T.; Cook, D.G. Plasma vitamin C levels in men and women from different ethnic backgrounds living in England. Int. J. Epidemiol. 1999, 28, 450–455. [Google Scholar] [CrossRef] [Green Version]
- Rowe, S.; Carr, A.C. Global Vitamin C Status and Prevalence of Deficiency: A Cause for Concern? Nutrients 2020, 12, 2008. [Google Scholar] [CrossRef] [PubMed]
- May, J.M. The SLC23 family of ascorbate transporters: Ensuring that you get and keep your daily dose of vitamin C. Br. J. Pharmacol. 2011, 164, 1793–1801. [Google Scholar] [CrossRef] [Green Version]
- Langlois, M.R.; Delanghe, J.R.; De Buyzere, M.L.; Bernard, D.R.; Ouyang, J. Effect of haptoglobin on the metabolism of vitamin C. Am. J. Clin. Nutr. 1997, 66, 606–610. [Google Scholar] [CrossRef]
- Michels, A.J.; Hagen, T.M.; Frei, B. Human genetic variation influences vitamin C homeostasis by altering vitamin C transport and antioxidant enzyme function. Annu. Rev. Nutr. 2013, 33, 45–70. [Google Scholar] [CrossRef] [Green Version]
- Cahill, L.E.; El-Sohemy, A. Haptoglobin genotype modifies the association between dietary vitamin C and serum ascorbic acid deficiency. Am. J. Clin. Nutr. 2010, 92, 1494–1500. [Google Scholar] [CrossRef] [Green Version]
- Delanghe, J.R.; Langlois, M.R.; De Buyzere, M.L.; Torck, M.A. Vitamin C deficiency and scurvy are not only a dietary problem but are codetermined by the haptoglobin polymorphism. Clin. Chem. 2007, 53, 1397–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langlois, M.R.; Delanghe, J.R. Biological and clinical significance of haptoglobin polymorphism in humans. Clin. Chem. 1996, 42, 1589–1600. [Google Scholar] [CrossRef] [Green Version]
- Carter, K.; Worwood, M. Haptoglobin: A review of the major allele frequencies worldwide and their association with diseases. Int. J. Lab. Hematol. 2007, 29, 92–110. [Google Scholar] [CrossRef] [PubMed]
- Nanri, A.; Kimura, Y.; Matsushita, Y.; Ohta, M.; Sato, M.; Mishima, N.; Sasaki, S.; Mizoue, T. Dietary patterns and depressive symptoms among Japanese men and women. Eur. J. Clin. Nutr. 2010, 64, 832–839. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; Pasco, J.A.; Mykletun, A.; Williams, L.J.; Hodge, A.M.; O’Reilly, S.L.; Nicholson, G.C.; Kotowicz, M.A.; Berk, M. Association of western and traditional diets with depression and anxiety in women. Am. J. Psychiatry 2010, 211, 55–68. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; Kremer, P.J.; Leslie, E.R.; Berk, M.; Patton, G.C.; Toumbourou, J.W.; Williams, J.W. Associations between diet quality and depressed mood in adolescents: Results from the Australian Healthy Neighbourhoods Study. Aust. N. Z. J. Psychiatry 2010, 44, 435–442. [Google Scholar] [CrossRef]
- Young, L.M.; Pipingas, A.; White, D.J.; Gauci, S.; Scholey, A. A systematic review and meta-analysis of B vitamin supplementation on depressive symptoms, anxiety, and stress: Effects on healthy and ‘at-risk’individuals. Nutrients 2019, 11, 2232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, J.; Gurbani, S. Association of Vitamin D Deficiency and Mood Disorders: A Systematic Review. Vitam. D Defic. 2019. [Google Scholar] [CrossRef] [Green Version]
- Jorm, A.F.; Rodgers, B.; Jacomb, P.A.; Christensen, H.; Henderson, S.; Korten, A.E. Smoking and mental health: Results from a community survey. Med. J. Aust. 1999, 170, 74–77. [Google Scholar] [CrossRef]
- Taylor, G.; McNeill, A.; Girling, A.; Farley, A.; Lindson-Hawley, N.; Aveyard, P. Change in mental health after smoking cessation: Systematic review and meta-analysis. BMJ 2014, 348, g1151. [Google Scholar] [CrossRef] [Green Version]
- Pearson, J.F.; Pullar, J.M.; Wilson, R.; Spittlehouse, J.K.; Vissers, M.; Skidmore, P.M.; Willis, J.; Cameron, V.A.; Carr, A.C. Vitamin C status correlates with markers of metabolic and cognitive health in 50-year-olds: Findings of the CHALICE cohort study. Nutrients 2017, 9, 831. [Google Scholar] [CrossRef]
- Lin, S.; Hsiao, Y.-Y.; Wang, M. Test Review: The Profile of Mood States, 2nd ed.; SAGE Publications: Los Angeles, CA, USA, 2014. [Google Scholar]
- Scott, K.M.; Sarfati, D.; Tobias, M.I.; Haslett, S.J. A challenge to the cross-cultural validity of the SF-36 health survey: Factor structure in Māori, Pacific and New Zealand European ethnic groups. Soc. Sci. Med. 2000, 51, 1655–1664. [Google Scholar] [CrossRef]
- Thumboo, J.; Fong, K.; Ng, T.; Leong, K.; Feng, P.; Thio, S.; Boey, M. Validation of the MOS SF-36 for quality of life assessment of patients with systemic lupus erythematosus in Singapore. J. Rheumatol. 1999, 26, 97–102. [Google Scholar] [PubMed]
- Ware, J.E., Jr.; Kosinski, M.; Gandek, B.; Aaronson, N.K.; Apolone, G.; Bech, P.; Brazier, J.; Bullinger, M.; Kaasa, S.; Leplège, A. The factor structure of the SF-36 Health Survey in 10 countries: Results from the IQOLA Project. J. Clin. Epidemiol. 1998, 51, 1159–1165. [Google Scholar] [CrossRef]
- Ware, J.E., Jr. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.-H. Review of the psychometric evidence of the perceived stress scale. Asian Nurs. Res. 2012, 6, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimmons, J.E.; Blanck, H.M.; Tohill, B.C.; Zhang, J.; Khan, L.K. Associations between body mass index and the prevalence of low micronutrient levels among US adults. Medscape Gen. Med. 2006, 8, 59. [Google Scholar]
- Ministry of Health. Annual Update of Key Results 2015/16: New Zealand Health Survey; Ministry of Health Wellington: Wellington, New Zealand, 2016.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria (All Required for Inclusion) | Exclusion Criteria (Only One Required for Exclusion) |
|---|---|
| Any gender aged 18–35 years | Taking prescription medication (within past three months) |
| Non-smoker | Allergy/intolerance to kiwifruit |
| Currently a student | Recent smoker (within past year) |
| Taking vitamin C supplements (within past three months) | |
| High fruit/juice and vegetable consumption (≥5 servings/day) | |
| Excessive alcohol consumption (>21 standard drinks/week) | |
| Serious health issues, such as diabetes mellitus, kidney disease, bleeding disorders, or clinical depression | |
| Fainting due to fear of needles |
| Mean (SD) | Minimum | Maximum | |||
| Age | 21.13 (3.33) | 18.00 | 35.00 | ||
| SES | 4.72 (1.22) | 1.00 | 7.00 | ||
| Vitamin C in µmol/L | 54.90 (20.19) | 4.29 | 118.91 | ||
| Total mood disturbance | 9.88 (14.42) | −18.00 | 71.00 | ||
| Vitality | 60.93 (15.09) | 15.00 | 95.00 | ||
| Perceived stress | 5.31 (2.06) | 0.00 | 11.00 | ||
| n (% of sample) | |||||
| Gender | Female | 284 (67.78%) | |||
| Male | 135 (32.22%) | ||||
| Gender diverse | 0 (0.00%) | ||||
| Ethnicity | European | 206 (49.16%) | |||
| NZ European | 187 (44.63%) | ||||
| Other European | 19 (4.53%) | ||||
| Asian | 129 (30.78%) | ||||
| East Asian a | 68 (16.23%) | ||||
| Southeast Asian b | 34 (8.11%) | ||||
| Other Asian c | 27 (6.44%) | ||||
| Māori or Pasifika d | 38 (9.07%) | ||||
| Other Ethnicities | 46 (10.98%) | ||||
| Indian | 25 (5.97%) | ||||
| Multiple Ethnicities | 12 (2.86%) | ||||
| Middle Eastern | 4 (0.95%) | ||||
| African | 3 (0.72%) | ||||
| Not Specified | 2 (0.48%) | ||||
| Total Mood Disturbance | Vitality | Perceived Stress | |
|---|---|---|---|
| Unadjusted associations | b (SE) | b (SE) | b (SE) |
| Total Sample | 0.002 (0.035) | 0.013 (0.037) | −0.006 (0.005) |
| European | 0.006 (0.047) | 0.071 (0.052) | 0.003 (0.007) |
| East Asian | 0.033 (0.084) | 0.001 (0.086) | −0.006 (0.012) |
| Southeast/Other Asian | 0.150 (0.104) | −0.254 (0.099) * | 0.016 (0.015) |
| Māori/Pasifika | −0.138 (0.144) | 0.309 (0.167) † | −0.039 (0.021) † |
| Other | −0.066 (0.137) | 0.135 (0.112) | −0.019 (0.017) |
| Adjusted associations 1 | b (SE) | b (SE) | b (SE) |
| Total Sample | −0.010 (0.035) | 0.031 (0.037) | −0.008 (0.005) † |
| European | 0.019 (0.048) | 0.070 (0.053) | 0.004 (0.007) |
| East Asian | 0.022 (0.080) | 0.002 (0.086) | −0.009 (0.011) |
| Southeast/Other Asian | 0.119 (0.097) | −0.223 (0.095) * | 0.012 (0.014) |
| Māori/Pasifika | −0.138 (0.151) | 0.318 (0.174) † | −0.042 (0.021) † |
| Other | −0.114 (0.130) | 0.151 (0.116) | −0.026 (0.016) |
| Adjusted + Moderators 2 | b (SE) | b (SE) | b (SE) |
| European | 0.008 (0.073) | 0.121 (0.076) | −0.004 (0.010) |
| East Asian | 0.029 (0.107) | 0.058 (0.111) | −0.016 (0.015) |
| Southeast/Other Asian | 0.149 (0.121) | −0.188 (0.125) | 0.005 (0.017) |
| Māori/Pasifika | −0.130 (0.157) | 0.373 (0.163) * | −0.048 (0.022) * |
| Other | −0.092 (0.140) | 0.201 (0.118) † | −0.031 (0.016) * |
| Tension | Depression | Anger | Fatigue | Confusion | Vigor | |
|---|---|---|---|---|---|---|
| Unadjusted associations | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) |
| Total Sample | 0.004 (0.008) | −0.006 (0.006) | −0.012 (0.007) † | 0.013 (0.009) | 0.001 (0.008) | −0.001 (0.009) |
| European | 0.018 (0.012) | 0.005 (0.008) | −0.011 (0.008) | 0.000 (0.012) | 0.001 (0.011) | 0.007 (0.012) |
| East Asian | −0.012 (0.020) | −0.006 (0.018) | 0.005 (0.017) | 0.011 (0.021) | 0.007 (0.020) | −0.029 (0.022) |
| Southeast/Other Asian | 0.028 (0.023) | 0.001 (0.019) | −0.007 (0.020) | 0.061 (0.032) † | 0.046 (0.022) * | −0.021 (0.026) |
| Māori/Pasifika | −0.043 (0.035) | −0.007 (0.021) | −0.007 (0.029) | −0.017 (0.042) | −0.037 (0.031) | 0.027 (0.036) |
| Other | 0.012 (0.031) | −0.010 (0.025) | −0.014 (0.027) | 0.010 (0.029) | −0.014 (0.029) | 0.049 (0.027) † |
| Adjusted associations 1 | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) |
| Total Sample | 0.002 (0.008) | −0.006 (0.006) | −0.011 (0.007) † | 0.010 (0.009) | −0.002 (0.008) | 0.003 (0.009) |
| European | 0.021 (0.012) † | 0.009 (0.008) | −0.008 (0.008) | 0.001 (0.013) | 0.004 (0.011) | 0.008 (0.013) |
| East Asian | −0.015 (0.019) | −0.008 (0.017) | 0.003 (0.017) | 0.010 (0.022) | 0.004 (0.018) | −0.027 (0.022) |
| Southeast/Other Asian | 0.021 (0.022) | −0.003 (0.018) | −0.009 (0.020) | 0.054 (0.032) † | 0.043 (0.022) † | −0.012 (0.026) |
| Māori/Pasifika | −0.037 (0.036) | −0.007 (0.022) | −0.014 (0.029) | −0.022 (0.044) | −0.031 (0.032) | 0.027 (0.038) |
| Other | −0.003 (0.030) | −0.016 (0.024) | −0.017 (0.027) | 0.005 (0.029) | −0.029 (0.027) | 0.055 (0.028) † |
| Adjusted + Moderators 2 | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) |
| European | 0.026 (0.018) | −0.002 (0.013) | −0.012 (0.014) | −0.008 (0.020) | 0.011 (0.016) | 0.006 (0.018) |
| East Asian | −0.005 (0.026) | −0.016 (0.019) | 0.002 (0.020) | 0.001 (0.029) | 0.016 (0.024) | −0.030 (0.027) |
| Southeast/Other Asian | 0.037 (0.029) | −0.010 (0.022) | −0.011 (0.023) | 0.051 (0.032) | 0.057 (0.027) * | −0.025 (0.030) |
| Māori/Pasifika | −0.031 (0.038) | −0.018 (0.028) | −0.010 (0.030) | −0.027 (0.042) | −0.021 (0.034) | 0.022 (0.040) |
| Other | 0.013 (0.028) | −0.022 (0.021) | −0.018 (0.022) | −0.002 (0.031) | −0.013 (0.025) | 0.050 (0.029) † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fletcher, B.D.; Flett, J.A.M.; Wickham, S.-R.; Pullar, J.M.; Vissers, M.C.M.; Conner, T.S. Initial Evidence of Variation by Ethnicity in the Relationship between Vitamin C Status and Mental States in Young Adults. Nutrients 2021, 13, 792. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030792
Fletcher BD, Flett JAM, Wickham S-R, Pullar JM, Vissers MCM, Conner TS. Initial Evidence of Variation by Ethnicity in the Relationship between Vitamin C Status and Mental States in Young Adults. Nutrients. 2021; 13(3):792. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030792
Chicago/Turabian StyleFletcher, Benjamin D., Jayde A. M. Flett, Shay-Ruby Wickham, Juliet M. Pullar, Margreet C. M. Vissers, and Tamlin S. Conner. 2021. "Initial Evidence of Variation by Ethnicity in the Relationship between Vitamin C Status and Mental States in Young Adults" Nutrients 13, no. 3: 792. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030792