
Body Composition, Dietary Intake and the Risk of Low Energy Availability in Elite-Level Competitive Rhythmic Gymnasts

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Body Composition
2.2. Nutrition Analysis
2.3. Physical Activity-Related and Basal Energy Expenditure
2.4. LEA Calculation
2.5. Statistical Analyses
3. Results
3.1. Body Composition
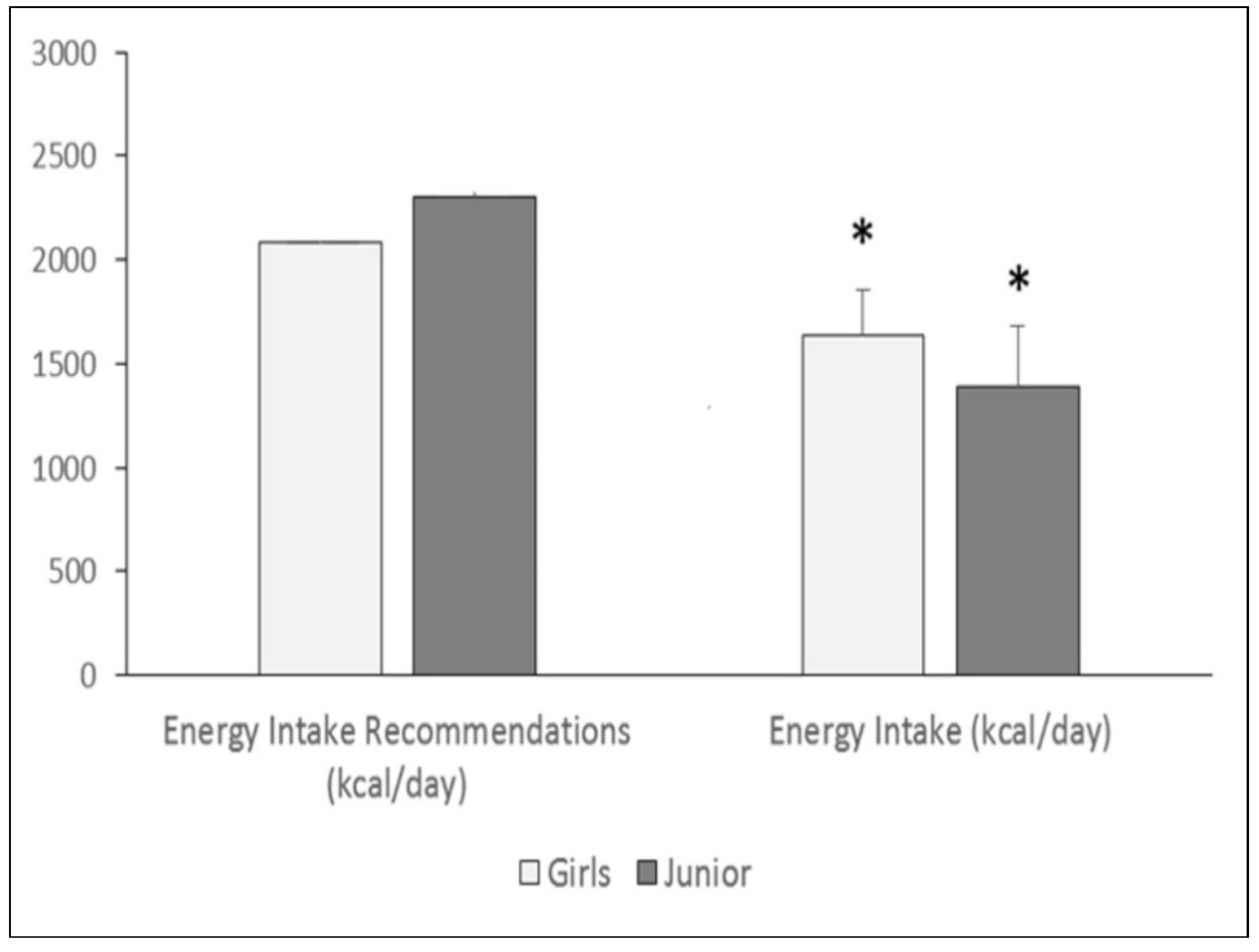
3.2. Nutrition Survey
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aerenhouts, D.; Deriemaeker, P.; Hebbelinck, M.; Clarys, P. Energy and macronutrient intake in adolescent sprint athletes: A follow-up study. J. Sports Sci. 2011, 29, 73–82. [Google Scholar] [CrossRef]
- Edouard, P.; Steffen, K.; Junge, A.; Leglise, M.; Soligard, T.; Engebretsen, L. Gymnastics injury incidence during the 2008, 2012 and 2016 Olympic Games: Analysis of prospectively collected surveillance data from 963 registered gymnasts during Olympic Games. Br. J. Sports Med. 2018, 52, 475–481. [Google Scholar] [CrossRef]
- Bacciotti, S.; Baxter-Jones, A.; Gaya, A.; Maia, J. The physique of elite female artistic gymnasts: A systematic re-view. J. Hum. Kinet. 2017, 58, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Georgopoulos, N.A.; Markou, K.B.; Theodoropoulou, A.; Vagenakis, G.A.; Benardot, D.; Leglise, M.; Dimopoulos, J.C.A.; Vagenakis, A.G. Height velocity and skeletal maturation in elite female rhythmic gymnasts. J. Clin. Endocrinol. Metab. 2001, 86, 5159–5164. [Google Scholar] [CrossRef]
- Bass, S.; Bradney, M.; Pearce, G.; Hendrich, E.; Inge, K.; Stuckey, S.; Lo, S.K.; Seeman, E. Short stature and delayed puberty in gymnasts: Influence of selection bias on leg length and the duration of training on trunk length. J. Pediatr. 2000, .136, 149–155. [Google Scholar] [CrossRef]
- Law, M.P.; Côté, J.; Ericsson, K.A. Characteristics of expert development in rhythmic gymnastics: A retrospective study. Int. J. Sport Exerc. Psychol. 2007, 5, 82–103. [Google Scholar] [CrossRef] [Green Version]
- Caine, D.; Lewis, R.; O’Connor, P.; Howe, W.; Bass, S. Does gymnastics training inhibit growth of females? Clin. J. Sport Med. 2001, 11, 260–270. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine joint position statement. Nutrition and athletic performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar] [CrossRef]
- Silva, M.-R.G.; Paiva, T. Poor precompetitive sleep habits, nutrients’ deficiencies, inappropriate body composition and athletic performance in elite gymnasts. Eur. J. Sport Sci. 2015, 16, 726–735. [Google Scholar] [CrossRef]
- Statuta, S.M.; Asif, I.M.; Drezner, J.A. Relative energy deficiency in sport (RED-S). Br. J. Sports Med. 2017, 51, 1570–1571. [Google Scholar] [CrossRef]
- Loucks, A.B.; Kiens, B.; Wright, H.H. Energy availability in athletes. J. Sports Sci. 2011, 29, S7–S15. [Google Scholar] [CrossRef]
- Logue, D.; Madigan, S.M.; Delahunt, E.; Heinen, M.; McDonnell, S.J.; Corish, C.A. Low energy availability in athletes: A review of prevalence, dietary patterns, physiological health, and sports performance. Sports Med. 2018, 48, 73–96. [Google Scholar] [CrossRef]
- Wasserfurth, P.; Palmowski, J.; Hahn, A.; Krüger, K. Reasons for and Consequences of Low Energy Availability in Female and Male Athletes: Social Environment, Adaptations, and Prevention. Sports Med. Open 2020, 6, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, E.J.; Hume, P.A. Biomechanical approaches to identify and quantify injury mechanisms and risk factors in women’s artistic gymnastics. Biomechanical approaches to identify and quantify injury. Sports Biomech. 2012, 11, 324–341. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.; Naka, T. Comparison of bone metabolism based on the different ages and competition levels of junior and high school female rhythmic gymnasts. J. Exerc. Nutr. Biochem. 2017, 21, 9–15. [Google Scholar] [CrossRef]
- Meng, K.; Quiu, J.; Benardot, D.; Carr, A.; Yi, L.; Wang, J.; Liang, Y. The risk of low energy availability in Chinese elite and recreational female aesthetic sports athletes. J. Int. Soc. Sports. Nutr. 2020, 17, 13. [Google Scholar] [CrossRef] [Green Version]
- Avila-Carvalho, L.; Klentrou, P.; Palomero, M.L.; Lebre, E. Body composition profile of elite group rhythmic gymnasts. Sci. Gymnast. J. 2012, 4, 21–32. [Google Scholar]
- D’Alessandro, C.; Morelli, E.; Evangelisti, I.; Galetta, F.; Franzoni, F.; Lazzeri, D.; Piazza, M.; Cupisti, A. Profiling the diet and body composition of subelite adolescent rhythmic gymnasts. Pediatr. Exerc. Sci. 2007, 19, 215–227. [Google Scholar] [CrossRef]
- Klentrou, P.; Plyley, M. Onset of puberty, menstrual frequency, and body fat in elite rhythmic gymnasts compared with normal controls. Br. J. Sports Med. 2003, 37, 490–494. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group. Assessment of differences in linear growth among populations in the WHO Multicentre Growth Reference Study. Acta Pædiatr. Suppl. 2006, 450, 56–65. [Google Scholar] [CrossRef]
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, L. International Standards for Anthropometric Assessment; The International Society for the Advancement of Kim Anthropometric (ISAK): Potchefsroom, South Africa, 2006. [Google Scholar]
- Mielgo-Ayuso, J.; Collado, P.S.; Urdampilleta, A.; Martínez-Sanz, J.M.; Seco, J. Changes induced by diet and nutritional intake in the lipid profile of female professional volleyball players after 11 weeks of training. J. Int. Soc. Sports Nutr. 2013, 10, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potgieter, S. Sport nutrition: A review of the latest guidelines for exercise and sport nutrition from the American College of Sport Nutrition, the International Olympic Committee and the International Society for Sports Nutrition. S. Afr. J. Clin. Nutr. 2013, 26, 6–16. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, Á.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos [Food Composition Tables]; Pirámide Ed.: Madrid, Spain, 2005. [Google Scholar]
- Carbajal, Á. Ingestas recomendadas de energίa y nutrientes. In Nutrición y Dietética (Revisited 2013); Garcίa-Arias, M.T., Garcίa-Fernández, M.C., Eds.; Secretariado de Publicaciones y Medios Audiovisuales, Universidad de León: León, Spain, 2003; pp. 1–26. Available online: https://www.ucm.es/data/cont/docs/458-2013-07-24-CARBAJAL-IR-2003-ISBN-84-9773-023-2-rev2013.pdf (accessed on 30 April 2021).
- Purcell, L.K.; Canadian Paediatric Society; Paediatric Sports; Exercise Medicine Section. Sport nutrition for young athletes. Paediatr. Child. Health 2013, 18, 200–202. [Google Scholar] [CrossRef] [PubMed]
- EFSA (European Food Safety Authority). Dietary Reference Values for Nutrients Summary Report; European Food Safety Authority: Parma, Italy, 2017; Volume 98, p. e15121. [Google Scholar]
- Zanders, B.R.; Currier, B.; Harty, P.S.; Zabriskie, H.; Smith, C.R.; Stecker, R.A.; Richmond, S.R.; Jagim, A.; Kerksick, C.M. Changes in Energy Expenditure, Dietary Intake, and Energy Availability Across an Entire Collegiate Women’s Basketball Season. J. Strength Cond. Res. 2021, 35, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Sjöström, M.; Yngve, A.; Poortvliet, E.; Nilsson, A.; Froberg, K.; Wedderkopp, N.; Westerterp, K. Physical activity assessed by activity monitor and doubly labeled water in children. Med. Sci. Sports Exerc. 2001, 33, 275–281. [Google Scholar] [CrossRef]
- Silva, M.-R.G.; Paiva, T. Low energy availability and low body fat of female gymnasts before an international competition. Eur. J. Sport Sci. 2014, 15, 591–599. [Google Scholar] [CrossRef]
- Silva, M.-R.G.; Silva, H.-H. Comparison of body composition and nutrients’ deficiencies between Portuguese rink-hockey players. Eur. J. Nucl. Med. Mol. Imaging 2016, 176, 41–50. [Google Scholar] [CrossRef]
- Otis, C.L.; Drinkwater, B.; Johnson, M.; Loucks, A.; Wilmore, J. ACSM Position Stand: The Female Athlete Triad. Med. Sci. Sports Exerc. 1997, 29, i–ix. [Google Scholar] [CrossRef]
- Weimann, E. Gender-related differences in elite gymnasts: The female athlete triad. J. Appl. Physiol. 2002, 92, 2146–2152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, M.T.; Garrido, G.; Soriano, L.; Martínez, J.; Donoso, M.A.; Hernández, M. Estado nutricional en adolescentes deportistas. Rev. Esp. Pediatr. 2003, 59, 222–231. [Google Scholar]
- Sureira, T.M.; Amancio, O.S.; Braga, J.A.P. Influence of artistic gymnastics on iron nutritional status and exercise-induced hemolysis in female athletes. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 243–250. [Google Scholar] [CrossRef]
- Gómez-Campos, R.; Camargo, C.; Arruda, M.; Cossio-Bolanos, M.A. Physical Growth and Nutritional Status of Elite Rhythmic Gymnasts. Nutr. Clín. Diet. Hosp. 2013, 33, 31–37. [Google Scholar]
- Silva, M.R.; Paiva, T. Risk factors for precompetitive sleep behavior in elite female athletes. J. Sports. Med. Phys. Fitness. 2019, 59, 708–716. [Google Scholar] [CrossRef] [PubMed]
- San Mauro Martín, I.; Cevallos, V.; Pina Ordúñez, D.; Garicano Vilar, E. Aspectos nutricionales, antropométricos y psicológicos en gimnasia rítmica. Nutr. Hosp. 2016, 33, 383. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.O.A.; Calitri, R.; Bloodworth, A.; McNamee, M. Understanding Eating Disorders in Elite Gymnastics. Clin. Sports Med. 2016, 35, 275–292. [Google Scholar] [CrossRef]
- Thompson, A.; Petrie, T.; Anderson, C. Eating disorders and weight control behaviors change over a collegiate sport season. J. Sci. Med. Sport 2017, 20, 808–813. [Google Scholar] [CrossRef]
- Ávila-Carvalho, L.; Klentrou, P.; Palomero, M.D.L.; Lebre, E. Anthropometric profiles and age at menarche in elite group rhythmic gymnasts according to their chronological age. Sci. Sports 2013, 28, 172–180. [Google Scholar] [CrossRef]
- Batista, A.; Garganta, R.; Ávila-Carvalho, L. Strength in young rhythmic gymnasts. J. Hum. Sport Exerc. 2017, 12, 1162–1175. [Google Scholar] [CrossRef] [Green Version]
- Arriaza, E.; Rodríguez, C.; Carrasco, C.; Mardones, C.; Niedmann, L.; López-Fuenzalida, A. Anthropometric Characteristics of Elite Rhythmic Gymnasts. Int. J. Morphol. 2016, 34, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Batista, A.; Garganta, R.; Ávila-Carvalho, L. Morphological characteristics and biological maturation of Brazilian and Portuguese gymnasts. Int. J. Morphol. 2019, 37, 561–567. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 30 April 2021).
- Douda, H.T.; Toubekis, A.G.; Avloniti, A.A.; Tokmakidis, S.P. Physiological and anthropometric determinants of rhythmic gymnastics performance. Int. J. Sports Physiol. Perform. 2008, 3, 41–54. [Google Scholar] [CrossRef] [Green Version]
- Theodoropoulou, A.; Markou, K.B.; Vagenakis, G.A.; Benardot, D.; Leglise, M.; Kourounis, G.; Vagenakis, A.G.; Georgopoulos, N.A. Delayed but normally progressed puberty is more pronounced in artistic compared with rhythmic elite gymnasts due to the intensity of training. J. Clin. Endocrinol. Metab. 2005, 90, 6022–6027. [Google Scholar] [CrossRef] [Green Version]
- Markou, K.B.; Mylonas, P.; Theodoropoulou, A.; Kontogiannis, A.; Leglise, M.; Vagenakis, A.G.; Georgopoulos, N.A. The influence of intensive physical exercise on bone acquisition in adolescent elite female and male artistic gymnasts. J. Clin. Endocrinol. Metab. 2004, 89, 4383–4387. [Google Scholar] [CrossRef] [Green Version]
- Gibson, J.C.; Stuart-Hill, L.; Martin, S.; Gaul, C. Nutrition status of junior elite Canadian female soccer athletes. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.A.; Wiens, K.P.; Erdman, K.A. Dietary intakes and supplement use in pre-adolescent and adolescent Canadian athletes. Nutrients 2016, 8, 526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desbrow, B.; McCormack, J.; Burke, L.M.; Cox, G.R.; Fallon, K.; Hislop, M.; Logan, R.; Marino, N.; Sawyer, S.M.; Shaw, G.; et al. Sports Dietitians Australia Position Statement: Sports nutrition for the adolescent athlete. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 570–584. [Google Scholar] [CrossRef] [PubMed]
- Muia, E.N.; Wright, H.H.; Onywera, V.O.; Kuria, E.N. Adolescent elite Kenyan runners are at risk for energy deficiency, menstrual dysfunction and disordered eating. J. Sports Sci. 2016, 34, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Roupas, N.D.; Maimoun, L.; Mamali, I.; Coste, O.; Tsouka, A.; Mahadea, K.K.; Mura, T.; Philibert, P.; Gaspari, L.; Mariano-Goulart, D.; et al. Salivary adiponectin levels are associated with training intensity but not with bone mass or reproductive function in elite Rhythmic Gymnasts. Peptides 2014, 51, 80–85. [Google Scholar] [CrossRef]
- Kapczuk, K. Elite athletes and pubertal delay. Minerva. Pediatr. 2017, 69, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Di Cagno, A.; Marchetti, M.; Battaglia, C.; Giombini, A.; Calcagno, G.; Fiorilli, G.; Piazza, M.; Pigozzi, F.; Borrione, P. Is menstrual delay a serious problem for elite rhythmic gymnasts. J. Sports Med. Phys. Fit. 2012, 52, 647–653. [Google Scholar]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Carter, S.; Constantini, N.; Lebrun, C.; Meyer, N.; Sherman, R.; Steffen, K.; Budgett, R.; et al. The IOC consensus statement: Beyond the Female Athlete Triad--Relative Energy Deficiency in Sport (RED-S). Br. J. Sports. Med. 2014, 48, 491–497. [Google Scholar] [CrossRef]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.; Meyer, N.; et al. International Olympic Committee (IOC) Consensus Statement on Relative Energy Deficiency in Sport (RED-S): 2018 Update. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 316–331. [Google Scholar] [CrossRef] [Green Version]
- Tenforde, A.S.; Carlson, J.L.; Sainani, K.L.; Chang, A.O.; Kim, J.H.; Golden, N.H.; Fredericson, M. Sport and Triad Risk Factors Influence Bone Mineral Density in Collegiate Athletes. Med. Sci. Sports Exerc. 2018, 50, 2536–2543. [Google Scholar] [CrossRef]
- Nazem, T.G.; Ackerman, K.E. The Female Athlete Triad. Sports Health A Multidiscip. 2012, 4, 302–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joy, E.; Kussman, A.; Nattiv, A. 2016 update on eating disorders in athletes: A comprehensive narrative review with a focus on clinical assessment and management. Br. J. Sports Med. 2016, 50, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whyte, H.E.; Findlay, S.M.; Canadian Paediatric Society; Adolescent Health Committee. Dieting in adolescence. J. Paediatr. Child Health 2004, 9, 487–491. [Google Scholar] [CrossRef] [Green Version]
- Aguilo, A.; Lozano, L.; Tauler, P.; Nafría, M.; Colom, M.; Martínez, S. Nutritional Status and Implementation of a Nutritional Education Program in Young Female Artistic Gymnasts. Nutrients 2021, 13, 1399. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.M.; Hawley, J.A.; Wong, S.H.S.; Jeukendrup, A.E. Carbohydrates for training and competition. J. Sports Sci. 2011, 29, S17–S27. [Google Scholar] [CrossRef] [PubMed]
- Petrie, H.J.; Stover, E.A.; Horswill, C.A. Nutritional concerns for the child and adolescent competitor. Nutrition 2004, 20, 620–631. [Google Scholar] [CrossRef]
- Mazzulla, M.; Volterman, K.A.; Packer, J.E.; Wooding, D.J.; Brooks, J.C.; Kato, H.; Moore, D.R. Whole-body net protein balance plateaus in response to increasing protein intakes during post-exercise recovery in adults and adolescents. Nutr. Metab. 2018, 15, 62. [Google Scholar] [CrossRef] [PubMed]
- Aranceta-Bartrina, J.; Partearroyo, T.; López-Sobaler, A.M.; Ortega, R.M.; Varela-Moreiras, G.; Serra-Majem, L.; Pérez-Rodrigo, C. The Collaborative Group for the Dietary Guidelines for the Spanish Population (SENC) The Collaborative Group for the Dietary Guidelines for the Spanish Population (SENC) Updating the Food-Based Dietary Guidelines for the Spanish Population: The Spanish Society of Community Nutrition (SENC) Proposal. Nutrients 2019, 11, 2675. [Google Scholar] [CrossRef] [Green Version]
- Malina, R.M.; Bouchard, C.; Bar-Or, O. Growth, Maturation, and Physical Activity, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Koehler, K.; Braun, H.; Achtzehn, S.; Hildebrand, U.; Predel, H.-G.; Mester, J.; Schänzer, W. Iron status in elite young athletes: Gender-dependent influences of diet and exercise. Eur. J. Appl. Physiol. 2012, 112, 513–523. [Google Scholar] [CrossRef]
- Lovell, G. Vitamin D Status of Females in an Elite Gymnastics Program. Clin. J. Sport Med. 2008, 18, 159–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.M.; Ross, M.L.; Garvican-Lewis, L.A.; Welvaert, M.; Heikura, I.A.; Forbes, S.G.; Mirtschin, J.G.; Cato, L.E.; Strobel, N.; Sharma, A.P.; et al. Low carbohydrate, high fat diet impairs exercise economy and negates the performance benefit from intensified training in elite race walkers. J. Physio. 2017, 595, 2785–2807. [Google Scholar] [CrossRef] [Green Version]
- Drew, M.K.; Vlahovich, N.; Hughes, D.; Appaneal, R.; Peterson, K.; Burke, L.; Lundy, B.; Toomey, M.; Watts, D.; Lovell, G.; et al. A multifactorial evaluation of illness risk factors in athletes preparing for the Summer Olympic games. J. Sci. Med. Sport. 2017, 20, 745–750. [Google Scholar] [CrossRef]
- Mountjoy, M.; Sundgot-Borgen, J.K.; Burke, L.M.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, AK.; Meyer, NL.; et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. British. J. Sports Med. 2018, 52, 687–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tornberg, Å.B.; Melin, A.; Koivula, F.M.; Johansson, A.; Skouby, S.; Faber, J.; Sjödin, A. Reduced neuromuscular performance in amenorrheic elite endurance athletes. Med. Sci. Sports Exerc. 2017, 49, 2478–2485. [Google Scholar] [CrossRef]
- Melin, A.K.; Heikura, I.A.; Tenforde, A.; Mountjoy, M. Energy Availability in Athletics: Health, Performance, and Physique. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 152–164. [Google Scholar] [CrossRef]
- Logue, D.M.; Madigan, S.M.; Melin, A.; Delahunt, E.; Heinen, M.; Donnell, S.M.; Corish, C.A. Low Energy Availability in Athletes 2020: An Updated Narrative Review of Prevalence, Risk, Within-Day Energy Balance, Knowledge, and Impact on Sports Performance. Nutrients 2020, 12, 835. [Google Scholar] [CrossRef] [Green Version]
- Mata, F.; Valenzuela, P.L.; Gimenez, J.; Tur, C.; Ferreria, D.; Domínguez, R.; Sanchez-Oliver, A.J.; Martínez Sanz, J.M. Carbohydrate Availability and Physical Performance: Physiological Overview and Practical Recommendations. Nutrients 2019, 11, 1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stellingwerff, T.; Bovim, I.M.; Whitfield, J. Contemporary Nutrition Interventions to Optimize Performance in Middle-Distance Runners. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 106–116. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Pre-Teens (9–12 Years), n = 17 | Teens (13–18 Years), n = 13 | p | η2p |
|---|---|---|---|---|
| Height (cm) | 136.2 ± 11.1 | 159.8 ± 4.6 * | <0.001 | 0.597 |
| Body weight (kg) | 29.5 ± 6.4 | 46.8 ± 5.7 | <0.001 | 0.652 |
| BMI | 15.8 ± 1.6 | 18.0 ± 1.8 | 0.003 | 0.300 |
| BMI z-score | −0.80 ± 0.74 | −1.15 ± 1.18 | 0.348 | 0.035 |
| Waist circumference (cm) | 54.9 ± 3.7 | 66.0 ± 4.6 | <0.001 | 0.592 |
| Hip circumference (cm) | 67.9 ± 5.4 | 82.8 ± 5.6 * | <0.001 | 0.637 |
| WHR | 0.81 ± 0.03 | 0.82 ± 0.02 | 0.018 | 0.205 |
| Muscle mass (kg) | 12.5 ± 2.4 | 22.5 ± 2.3 * | <0.001 | 0.697 |
| Muscle mass (%) | 44.1 ± 2.4 | 46.8 ± 3.0 | 0.017 | 0.207 |
| Fat mass (kg) | 4.1 ± 1.6 | 7.1 ± 3.40 * | 0.003 | 0.294 |
| Fat mass (%) | 14.0 ± 3.8 | 14.3 ± 5.6 | 0.763 | 0.004 |
| Fat-free mass (kg) | 25.4 ± 5.6 | 41.2 ± 3.9 * | <0.001 | 0.698 |
| Fat-free mass (%) | 86.2 ± 3.8 | 85.7 ± 5.6 | 0.763 | 0.004 |
| Bone mineral content (kg) | 1.4 ± 0.2 | 2.4 ± 0.3 * | <0.001 | 0.719 |
| Bone mineral content (%) | 4.9 ± 0.3 | 5.1 ± 0.8 | 0.625 | 0.010 |
| Extracellular water content (kg) | 7.1 ± 1.5 | 11.4 ± 1.8 | <0.001 | 0.686 |
| Intracellular water content (kg) | 11.6 ± 2.5 | 18.8 ± 1.1 | <0.001 | 0.699 |
| Total Intake | % RDA † | % Below RDA | % Met RDA | % Exceeded RDA | |
|---|---|---|---|---|---|
| Energy (kcal) | |||||
| Pre-teen | 1640 ± 212 | 78.7 | 38.1 | 62.0 | 0.0 |
| Teen | 1388 ± 295 | 60.36 | 85.71 | 14.29 | 0.00 |
| Water (mL) | |||||
| Pre-teen | 1299 ± 244 | ||||
| Teen | 1303 ± 307 | ||||
| Protein (g) | |||||
| Pre-teen | 70.7 ± 13.9 | 208.1 | 0.00 | 0.00 | 100.0 |
| Teen | 73.6 ± 8.3 | 160.1 | 0.00 | 0.00 | 100.0 |
| Protein% kcal (10–15%) | |||||
| Pre-teen | 17.25 ± 3.38 | 0.0 | 20 | 80.0 | |
| Teen | 21.2 ± 2.4 * | 0.0 | 0.0 | 100.0 | |
| Fat (g) | |||||
| Pre-teen | 67.4 ± 10.2 | 88.2 | 20.0 | 80.0 | 0.0 |
| Teen | 50.6 ± 15.4 * | 60.04 | 85.71 | 14.29 | 0.00 |
| Fat% kcal (20–35%) | |||||
| Pre-teen | 37.0 ± 6.6 | 0.0 | 40.0 | 60.0 | |
| Teen | 32.8 ± 10.0 | 0.0 | 57.1 | 42.9 | |
| SFAs (g) | |||||
| Pre-teen | 19.8 ± 5.2 | 107.2 | 13.33 | 73.33 | 13.33 |
| Teen | 16.5 ± 8.2 * | 80.85 | 57.14 | 28.57 | 14.29 |
| MFAs (g) | |||||
| Pre-teen | 24.8 ± 5.7 | 53.6 | 86.67 | 13.33 | 0.00 |
| Teen | 20.1 ± 5.9 * | 39.26 | 100.0 | 0.00 | 0.00 |
| PFAs (g) | |||||
| Pre-teen | 6.6 ± 1.4 | 57.2 | 93.33 | 6.67 | 0.00 |
| Teen | 5.3 ± 1.1 | 41.10 | 100.0 | 0.00 | 0.00 |
| Cholesterol (mg) < 300 g | |||||
| Pre-teen | 235.0 ± 93.6 | - | 76.60 | 19.10 | |
| Teen | 249.4 ± 56.1 | - | 83.33 | 16.7 | |
| Carbohydrate (g) | |||||
| Pre-teen | 202.6 ± 29.9 | 70.1 | 73.33 | 26.67 | 0.00 |
| Teen | 169.6 ± 50.4 | 53.19 | 85.71 | 14.29 | 0.00 |
| Carbohydrate% kcal (>50%) | |||||
| Pre-teen | 49.4 ± 7.20 | 60.0 | 40.0 | 0.00 | |
| Teen | 48.9 ± 14.5 | 57.1 | 42.9 | 0.00 | |
| Fiber (g) | |||||
| Pre-teen | 13.8 ± 4.1 | 55.4 | 100.0 | 0.00 | 0.00 |
| Teen | 10.9 ± 1.7 | 43.43 | 100.0 | 0.00 | 0.00 |
| Pre-Teen (9–12 Years), n = 17 | Teen (13–18 Years), n = 13 | |
|---|---|---|
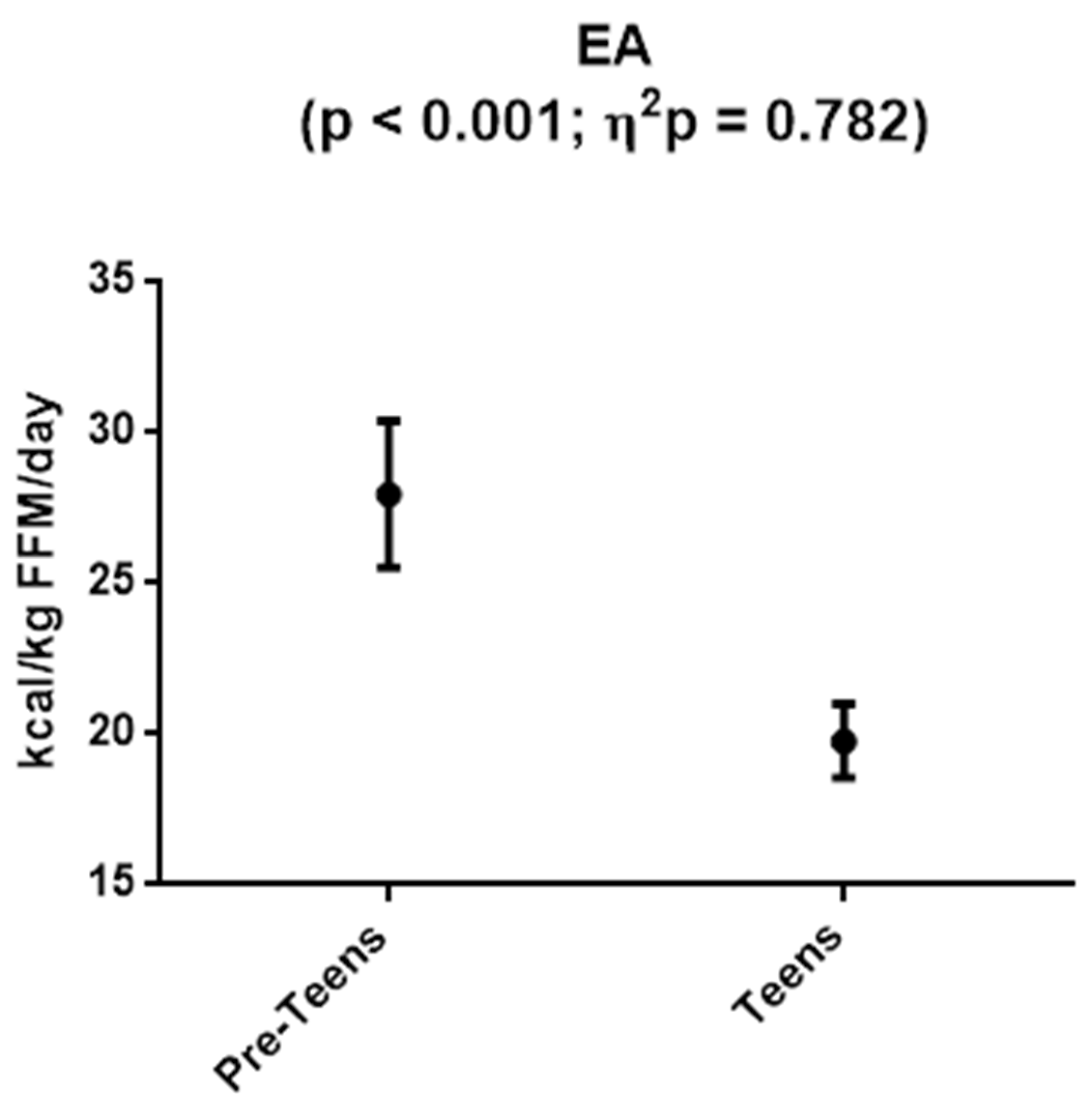
| Energy (kcal/kg FFM) | 66.9 ± 9.5 | 33.6 ± 8.0 * |
| Protein (g/kg BM) | 2.6 ± 0.6 | 1.6 ± 0.3 * |
| Carbohydrate (g/kg BM) | 7.4 ± 1.5 | 3.7 ± 1.3 * |
| Fat (g/kg BM) | 2.5 ± 0.6 | 1.2 ± 0.4 * |
| Pre-Teen (9–12 Years) (n = 17) | % RDA † | Teen (13–18 Years) (n = 13) | % RDA | ||
|---|---|---|---|---|---|
| Minerals | Na (mg) | 1617 ± 488 | - | 1612 ± 390 | - |
| K (mg) | 1999 ± 355 | 64.5 | 2184 ± 614 | 62.4 | |
| Ca (mg) | 831.2 ± 189.8 | 63.9 | 840.9 ± 267.5 | 64.6 | |
| Mg (mg) | 231.1 ± 29.6 | 77.0 | 252.8 ± 70.4 | 76.6 | |
| P (mg) | 1134 ± 188 | 94.5 | 1088 ± 213 | 90.6 | |
| Fe (mg) | 13.5 ± 4.6 | 75.0 | 11.1 ± 2.6 * | 61.7 | |
| Cu (mg) | 0.7 ± 0.1 | - | 0.6 ± 0.1 | - | |
| Zn (mg) | 7.9 ± 4.1 | 52.7 | 10.5 ± 5.0 | 70.0 | |
| Cl (mg) | 1132 ± 540 | - | 1262 ± 336 | - | |
| Mn (mg) | 2.4 ± 1.7 | - | 4.9 ± 4.8 | - | |
| Se (µg) | 52.0 ± 15.8 | 115.6 | 60.0 ± 14.8 | 120.0 | |
| I (µg) | 43.4 ± 17.0 | 37.7 | 80.1 ± 30.2 | 69.7 | |
| Vitamins | B1 (mg)thiamine | 1.3 ± 0.5 | 144.4 | 1.2 ± 0.2 | 120.0 |
| B2 (mg)riboflavin | 1.7 ± 0.4 | 121.4 | 1.6 ± 0.5 | 106.7 | |
| B6 (mg) | 4.1 ± 1.4 | 256.3 | 1.7 ± 0.3 * | 100.0 | |
| B12 (µg) | 7.3 ± 3.8 | 365.0 | 4.7 ± 0.9 * | 235.0 | |
| Folate (µg) | 222.4 ± 72.4 | 74.1 | 190.8 ± 49.3 | 47.5 | |
| Niacin (mg) | 19.4 ± 5.5 | 129.3 | 20.7 ± 2.6 | 121.8 | |
| C (mg) | 83.8 ± 41.4 | 139.7 | 68.9 ± 44.9 | 114.8 | |
| Pantothenic (mg) | 4.0 ± 1.8 | - | 4.1 ± 1.1 | - | |
| Biotin (mg) | 7.8 ± 3.2 | - | 4.0 ± 1.6 * | - | |
| Retinol (µg) | 670.6 ± 222.8 | 83.8 | 619.2 ± 364.7 | 77.4 | |
| D (µg) | 3.0 ± 2.9 | 20.0 | 3.7 ± 3.9 | 24.7 | |
| E (mg) | 7.8 ± 2.8 | 78.0 | 6.0 ± 1.9 | 52.2 | |
| Pre-Teen (9–12 Years) (n = 17) | Teen (13–18 Years) (n = 13) | p | |
|---|---|---|---|
| Adequate EA | 0 (0%) | 0 (0%) | 0.005 |
| Subclinical EA | 12 (70.6%) | 0 (0%) | |
| LEA | 2 (29.4%) | 13 (100%) | |
| Extreme LEA | 0 (0%) | 0 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villa, M.; Villa-Vicente, J.G.; Seco-Calvo, J.; Mielgo-Ayuso, J.; Collado, P.S. Body Composition, Dietary Intake and the Risk of Low Energy Availability in Elite-Level Competitive Rhythmic Gymnasts. Nutrients 2021, 13, 2083. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13062083
Villa M, Villa-Vicente JG, Seco-Calvo J, Mielgo-Ayuso J, Collado PS. Body Composition, Dietary Intake and the Risk of Low Energy Availability in Elite-Level Competitive Rhythmic Gymnasts. Nutrients. 2021; 13(6):2083. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13062083
Chicago/Turabian StyleVilla, María, José G. Villa-Vicente, Jesus Seco-Calvo, Juan Mielgo-Ayuso, and Pilar S. Collado. 2021. "Body Composition, Dietary Intake and the Risk of Low Energy Availability in Elite-Level Competitive Rhythmic Gymnasts" Nutrients 13, no. 6: 2083. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13062083