
Dietary Characteristics and Influencing Factors on Chinese Immigrants in Canada and the United States: A Scoping Review


Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources
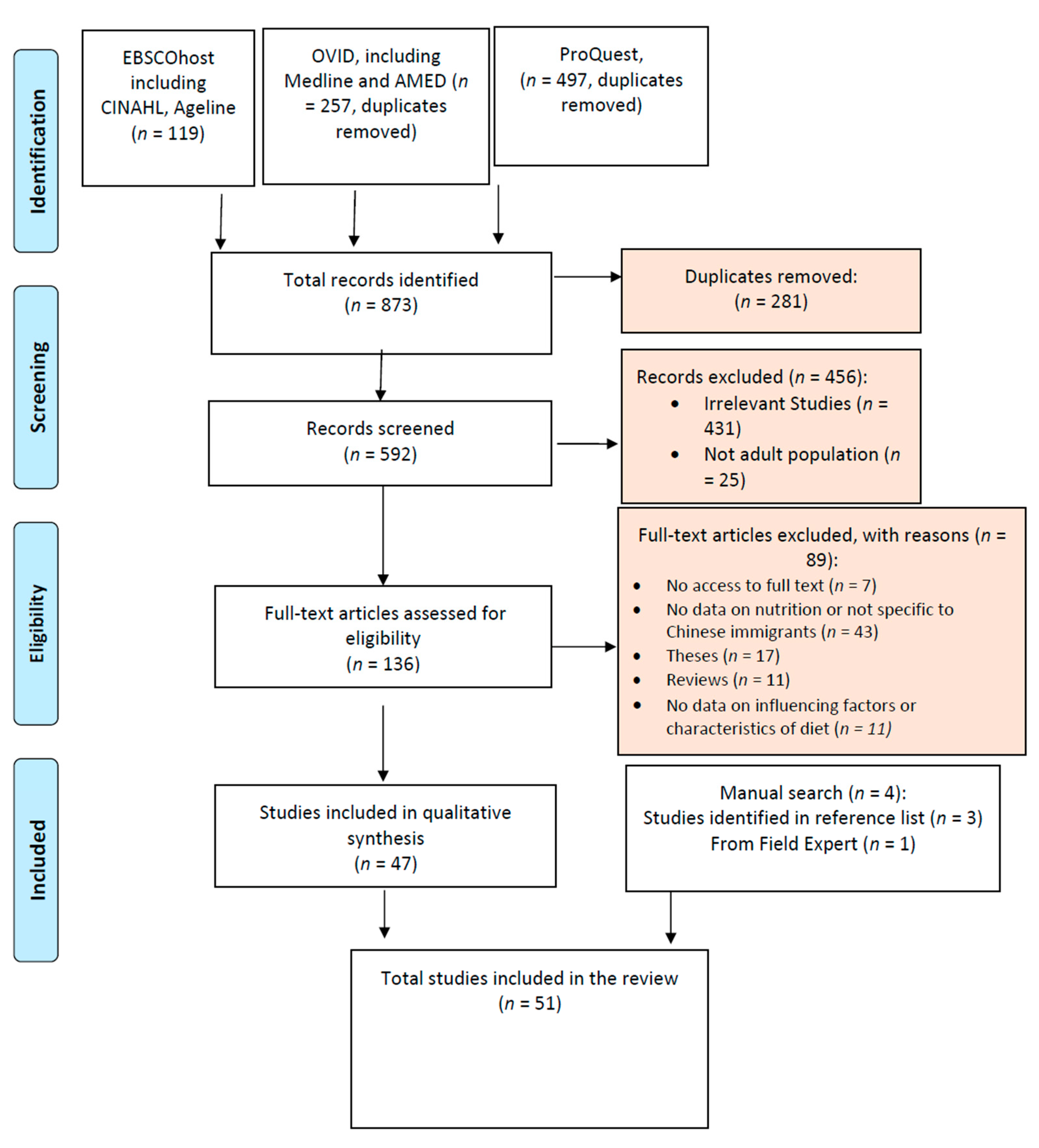
2.3. Search Strategy and Selection of Evidence
2.4. Quality Assessment
2.5. Data Extraction
2.6. Synthesis of Results
3. Results
3.1. Characteristics of Included Studies
3.2. Dietary Characteristics
3.2.1. Food Consumption
3.2.2. Macronutrient Intake
3.2.3. Micronutrient and Caloric Intake
3.2.4. Dietary Changes since Immigration
3.3. Factors Influencing Dietary Behaviours
3.3.1. Acculturation and Its Associations with Diet
3.3.2. Individual Factors
3.3.3. Familial Factors
3.3.4. Community Factors
4. Discussions
4.1. Summary of Findings
4.2. Dietary Characteristics
4.3. Influencing Factors
4.4. Implications
4.5. Limitations of This Review and Recommendations for Future Studies
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Government of Canada. Immigration and Ethnocultural Diversity Statistics; Statistics Canada: Ottawa, ON, Canada, 2019. Available online: https://www.statcan.gc.ca/en/subjects-start/immigration_and_ethnocultural_diversity (accessed on 20 May 2022).
- Estrada, C.E.; Batalova, J. Chinese Immigrants in the United States. 2020. Available online: migrationpolicy.org (accessed on 20 May 2022).
- Suryadinata, L. Migration, Indigenization, and Interaction: Chinese Overseas and Globalization; World Scientific: Singapore, 2011; 335p. [Google Scholar]
- Pearce, R.R.; Lin, Z. Chinese American post-secondary achievement and attainment: A cultural and structural analysis. Educ. Rev. 2007, 59, 19–36. [Google Scholar] [CrossRef]
- Washington, G.; Wang-Letzkus, M.F. Self-care practices, health beliefs, and attitudes of older diabetic Chinese Americans. J. Health Hum. Serv. Adm. 2009, 32, 305–323. [Google Scholar] [PubMed]
- Nestler, G. Traditional Chinese medicine. Med. Clin. 2002, 86, 63–73. [Google Scholar] [CrossRef]
- Higginbottom, G.M.A.; Vallianatos, H.; Shankar, J.; Safipour, J.; Davey, C. “Immigrant women’s food choices in pregnancy: Perspectives from women of Chinese origin in Canada”: Corrigendum. Ethn. Health 2018, 23, 914. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Yi, S.S.; Ahn, J.; Kwon, S.C.; Wylie-Rosett, J. Dietary Patterns in Chinese Americans are Associated with Cardiovascular Disease Risk Factors, the Chinese American Cardiovascular Health Assessment (CHA CHA). J. Immigr. Minor. Health 2019, 21, 1061–1069. [Google Scholar] [CrossRef]
- Roberts, C.K.; Barnard, R.J. Effects of exercise and diet on chronic disease. J. Appl. Physiol. 2005, 98, 3–30. [Google Scholar] [CrossRef] [Green Version]
- Sanou, D.; O’Reilly, E.; Ngnie-Teta, I.; Batal, M.; Mondain, N.; Andrew, C.; Newbold, B.K.; Bourgeault, I. Acculturation and Nutritional Health of Immigrants in Canada: A Scoping Review. J. Immigr. Minor. Health 2014, 16, 24–34. [Google Scholar] [CrossRef] [Green Version]
- LeCroy, M.N.; Stevens, J. Dietary intake and habits of South Asian immigrants living in Western countries. Nutr. Rev. 2017, 75, 391–404. [Google Scholar] [CrossRef]
- Elshahat, S.; Moffat, T. Dietary practices among Arabic-speaking immigrants and refugees in Western societies: A scoping review. Appetite 2020, 154, 104753. [Google Scholar] [CrossRef]
- Deng, F.; Zhang, A.; Chan, C.B. Acculturation, Dietary Acceptability, and Diabetes Management among Chinese in North America. Front. Endocrinol. 2013, 4, 108. [Google Scholar] [CrossRef] [Green Version]
- Li-Geng, T.; Kilham, J.; McLeod, K.M. Cultural Influences on Dietary Self-Management of Type 2 Diabetes in East Asian Americans: A Mixed-Methods Systematic Review. Health Equity 2020, 4, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Theories for social epidemiology in the 21st century: An ecosocial perspective. Int. J. Epidemiol. 2001, 30, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Zou, P. Facilitators and Barriers to Healthy Eating in Aged Chinese Canadians with Hypertension: A Qualitative Exploration. Nutrients 2019, 11, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Critical Appraisal Skills Programme. CASP Checklists. 2017. Available online: http://www.casp-uk.net/casp-tools-checklists (accessed on 5 May 2022).
- A Rodriguez, L.; Jin, Y.; A Talegawkar, S.; Otto, M.C.D.O.; Kandula, N.R.; Herrington, D.M.; Kanaya, A.M. Differences in Diet Quality among Multiple US Racial/Ethnic Groups from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study and the Multi-Ethnic Study of Atherosclerosis (MESA). J. Nutr. 2020, 150, 1509–1515. [Google Scholar] [CrossRef]
- Chai, S.C.; Jiang, H.; Papas, M.A.; Fang, C.-S.; Setiloane, K.T. Acculturation, diet, and psychological health among Asian students. J. Am. Coll. Health 2019, 67, 433–440. [Google Scholar] [CrossRef]
- Kirshner, L.; Yi, S.; Wylie-Rosett, J.; Matthan, N.R.; Beasley, J. Acculturation and Diet Among Chinese American Immigrants in New York City. Curr. Dev. Nutr. 2019, 4, nzz124. [Google Scholar] [CrossRef]
- An, Z. Diet-specific social support, dietary acculturation, and self-efficacy among Chinese living in the United States. J. Int. Intercult. Commun. 2018, 11, 136–153. [Google Scholar] [CrossRef]
- Liu, L.W. From shopping to eating: Food safety practices among Chinese immigrants in Canada. Int. J. Anthr. Ethnol. 2017, 1, 4. [Google Scholar] [CrossRef]
- Lu, C.; McGinn, M.K.; Xu, X.; Sylvestre, J. Living in Two Cultures: Chinese Canadians’ Perspectives on Health. J. Immigr. Minor. Health 2017, 19, 423–429. [Google Scholar] [CrossRef]
- Zou, P.; Dennis, C.-L.; Cindy-Lee, D.; Parry, M. Hypertension Prevalence, Health Service Utilization, and Participant Satisfaction: Findings From a Pilot Randomized Controlled Trial in Aged Chinese Canadians. Inq. J. Health Care Organ. Provis. Financ. 2017, 54, 46958017724942. [Google Scholar] [CrossRef]
- Yi, S.S.; Thorpe, L.E.; Zanowiak, J.M.; Trinh-Shevrin, C.; Islam, N.S. Clinical Characteristics and Lifestyle Behaviors in a Population-Based Sample of Chinese and South Asian Immigrants With Hypertension. Am. J. Hypertens. 2016, 29, 941–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, M.; Wright, D.J.; Fang, C.Y. Acculturation and Dietary Change Among Chinese Immigrant Women in the United States. J. Immigr. Minor. Health 2015, 17, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Corlin, L.; Woodin, M.; Thanikachalam, M.; Lowe, L.; Brugge, D. Evidence for the healthy immigrant effect in older Chinese immigrants: A cross-sectional study. BMC Public Health 2014, 14, 603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyatt, L.C.; Trinh-Shevrin, C.; Islam, N.S.; Kwon, S. Health-Related Quality of Life and Health Behaviors in a Population-Based Sample of Older, Foreign-Born, Chinese American Adults Living in New York City. Health Educ. Behav. 2014, 41 (Suppl. 1), 98S–107S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adekunle, B.; Filson, G.; Sethuratnam, S. Immigration and Chinese food preferences in the Greater Toronto Area. Int. J. Consum. Stud. 2013, 37, 658–665. [Google Scholar] [CrossRef]
- Wong, S.S.; Dixon, L.B.; Gilbride, J.A.; Kwan, T.W.; Stein, R.A. Measures of Acculturation are Associated with Cardiovascular Disease Risk Factors, Dietary Intakes, and Physical Activity in Older Chinese Americans in New York City. J. Immigr. Minor. Health 2013, 15, 560–568. [Google Scholar] [CrossRef]
- Tam, C.Y.; Hislop, G.; Hanley, A.J.; Minkin, S.; Boyd, N.F.; Martin, L.J. Food, Beverage, and Macronutrient Intakes in Postmenopausal Caucasian and Chinese-Canadian Women. Nutr. Cancer 2011, 63, 687–698. [Google Scholar] [CrossRef]
- Tseng, M.; Fang, C.Y. Socio-economic position and lower dietary moderation among Chinese immigrant women in the USA. Public Health Nutr. 2012, 15, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Alonge, O.K.; Narendran, S.; Hobdell, M.H.; Bahl, S. Sugar consumption and preference among Mexican, Chinese, and Nigerian immigrants to Texas. Speéc. Care Dent. 2011, 31, 150–155. [Google Scholar] [CrossRef]
- Lv, N.; Brown, J.L. Impact of a Nutrition Education Program to Increase Intake of Calcium-Rich Foods by Chinese-American Women. J. Am. Diet. Assoc. 2011, 111, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Rosenmöller, D.L.; Gasevic, D.; Seidell, J.; A Lear, S. Determinants of changes in dietary patterns among Chinese immigrants: A cross-sectional analysis. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, C.Y.; Martin, L.J.; Hislop, G.; Hanley, A.J.; Minkin, S.; Boyd, N.F. Risk factors for breast cancer in postmenopausal Caucasian and Chinese-Canadian women. Breast Cancer Res. 2010, 12, R2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, M.; Fang, C.Y. Stress Is Associated with Unfavorable Patterns of Dietary Intake Among Female Chinese Immigrants. Ann. Behav. Med. 2011, 41, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, A.; Berhane, Z.; Tseng, M. Improved Dietary Variety and Adequacy but Lower Dietary Moderation with Acculturation in Chinese Women in the United States. J. Am. Diet. Assoc. 2010, 110, 457. [Google Scholar] [CrossRef] [Green Version]
- Bell, K.; Lee, J.; Ristovski-Slijepcevic, S. Perceptions of food and eating among Chinese patients with cancer: Findings of an ethnographic study. Cancer Nurs. 2009, 32, 118–126. [Google Scholar] [CrossRef]
- Chesla, C.A.; Chun, K.M.; Kwan, C.M. Cultural and Family Challenges to Managing Type 2 Diabetes in Immigrant Chinese Americans. Diabetes Care 2009, 32, 1812–1816. [Google Scholar] [CrossRef] [Green Version]
- Kwok, S.; Mann, L.; Wong, K.; Blum, I. Dietary habits and health beliefs of Chinese Canadians. Can. J. Diet. Pr. Res. 2009, 70, 73–80. [Google Scholar] [CrossRef]
- Osypuk, T.L.; Roux, A.V.D.; Hadley, C.; Kandula, N.R. Are immigrant enclaves healthy places to live? The Multi-ethnic Study of Atherosclerosis. Soc. Sci. Med. 2009, 69, 110–120. [Google Scholar] [CrossRef] [Green Version]
- Hislop, T.G.; Tu, S.-P.; Teh, C.; Li, L.; Low, A.; Taylor, V.M.; Yasui, Y. Knowledge and Behaviour Regarding Heart Disease Prevention in Chinese Canadian Immigrants. Can. J. Public Health 2008, 99, 232–235. [Google Scholar] [CrossRef]
- Kandula, N.R.; Diez-Roux, A.V.; Chan, C.; Daviglus, M.L.; Jackson, S.A.; Ni, H.; Schreiner, P.J. Association of Acculturation Levels and Prevalence of Diabetes in the Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care 2008, 31, 1621–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.; Sylvestre, J.; Melnychuk, N.; Li, J. East Meets West: Chinese-Canadians’ Perspectives on Health and Fitness. Can. J. Public Health 2008, 99, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Taylor, V.M.; Yasui, Y.; Tu, S.P.; Neuhouser, M.L.; Li, L.; Woodall, E.; Acorda, E.; Cripe, S.M.; Hislop, T.G. Heart disease prevention among Chinese immigrants. J. Community Health: Publ. Health Promot. Dis. Prev. 2007, 32, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Babbar, R.K.; Handa, A.B.; Lo, C.-M.; Guttmacher, S.J.; Shindledecker, R.; Chung, W.; Fong, C.; Ho-Asjoe, H.; Chan-Ting, R.; Dixon, L.B. Bone Health of Immigrant Chinese Women Living in New York City. J. Community Health 2006, 31, 7–23. [Google Scholar] [CrossRef]
- Fang, J.; Foo, S.H.; Fung, C.; Wylie-Rosett, J.; Alderman, M.H. Stroke Risk among Chinese Immigrants in New York City. J. Immigr. Minor. Health 2006, 8, 387–393. [Google Scholar] [CrossRef]
- Walker, M.D.; Babbar, R.; Opotowsky, A.; McMahon, D.J.; Liu, G.; Bilezikian, J.P. Determinants of bone mineral density in Chinese-American women. Osteoporos. Int. 2007, 18, 471–478. [Google Scholar] [CrossRef]
- Liang, W.; Yuan, E.; Mandelblatt, J.S.; Pasick, R.J. How do older Chinese women view health and cancer screening? results from focus groups and implications for interventions. Ethn. Health 2004, 9, 283–304. [Google Scholar] [CrossRef]
- Lv, N.; Cason, K.L. Dietary pattern change and acculturation of Chinese Americans in Pennsylvania. J. Am. Diet. Assoc. 2004, 104, 771–778. [Google Scholar] [CrossRef]
- Lv, N.; Cason, K.L. Current Dietary Pattern and Acculturation of Chinese Americans in Pennsylvania. Top. Clin. Nutr. 2003, 18, 291–300. [Google Scholar] [CrossRef]
- Kelemen, L.E.; Anand, S.S.; Vuksan, V.; Yi, Q.; Teo, K.K.; Devanesen, S.; Yusuf, S. Development and evaluation of cultural food frequency questionnaires for South Asians, Chinese, and Europeans in North America. J. Am. Diet. Assoc. 2003, 103, 1178–1184. [Google Scholar] [CrossRef]
- Satia-Abouta, J.; Patterson, R.E.; Kristal, A.; Teh, C.; Tu, S.-P. Psychosocial Predictors of Diet and Acculturation in Chinese American and Chinese Canadian Women. Ethn. Health 2002, 7, 21–39. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Wan, P.; Hankin, J.; Tseng, C.-C.; Yu, M.C.; Pike, M.C. Adolescent and adult soy intake and risk of breast cancer in Asian-Americans. Carcinogenesis 2002, 23, 1491–1496. [Google Scholar] [CrossRef] [PubMed]
- Liou, D.; Contento, I.R. Usefulness of Psychosocial Theory Variables in Explaining Fat-Related Dietary Behavior in Chinese Americans: Association with Degree of Acculturation. J. Nutr. Educ. 2001, 33, 322–331. [Google Scholar] [CrossRef]
- A Satia, J.; E Patterson, R.; Kristal, A.R.; Hislop, T.G.; Pineda, M. A household food inventory for North American Chinese. Public Health Nutr. 2001, 4, 241–247. [Google Scholar] [CrossRef] [Green Version]
- A Satia, J.; E Patterson, R.; Kristal, A.R.; Hislop, T.; Yasui, Y.; Taylor, V.M. Development of scales to measure dietary acculturation among Chinese-Americans and Chinese-Canadians. J. Am. Diet. Assoc. 2001, 101, 548–553. [Google Scholar] [CrossRef]
- Satia, J.A.; Patterson, R.E.; Taylor, V.M.; Cheney, C.L.; Shiu-Thornton, S.; Chitnarong, K.; Kristal, A.R. Use of qualitative methods to study diet, acculturation, and health in Chinese-American women. American Dietetic Association. J. Am. Diet. Assoc. 2000, 100, 934–940. [Google Scholar] [CrossRef]
- Whittemore, A.S.; Kolonel, L.N.; Wu, A.H.; John, E.M.; Gallagher, R.P.; Howe, G.R.; Burch, J.D.; Hankin, J.; Dreon, D.M.; West, D.W.; et al. Prostate Cancer in Relation to Diet, Physical Activity, and Body Size in Blacks, Whites, and Asians in the United States and Canada. JNCI J. Natl. Cancer Inst. 1995, 87, 652–661. [Google Scholar] [CrossRef]
- Choi, E.S.K. The Prevalence of Cardiovascular Risk Factors Among Elderly Chinese Americans. Arch. Intern. Med. 1990, 150, 413–418. [Google Scholar] [CrossRef]
- Whittemore, A.S.; Wu-Williams, A.H.; Lee, M.; Zheng, S.; Gallagher, R.P.; A Jiao, D.; Zhou, L.; Wang, X.H.; Chen, K.; Jung, D. Diet, physical activity, and colorectal cancer among Chinese in North America and China. JNCI J. Natl. Cancer Inst. 1990, 82, 915–926. [Google Scholar] [CrossRef]
- Newman, J.M. Chinese Immigrant Food Habits: A Study of the Nature and Direction of Change; New York University: Ann Arbor, MI, USA, 1980; p. 149. [Google Scholar]
- Wang, K. Acculturation, Sociodemographic and Environmental Determinants of Dietary Intake among Asian Immigrants in the United States; Graduate School of Social Work, Boston University: Boston, MA, USA, 2017. [Google Scholar]
- Milani, G.P.; Silano, M.; Pietrobelli, A.; Agostoni, C. Junk food concept: Seconds out. Int. J. Obes. 2017, 41, 669. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; US Government Printing Office: Washington, DC, USA, 2020; Volume 164.
- Dai, C.-L.; Sharma, M.; Haider, T.; Sunchu, H. Fruit and Vegetable Consumption Behavior Among Asian Americans: A Thematic Analysis. J. Prim. Care Community Health 2021, 12, 2150132720984776. [Google Scholar] [CrossRef] [PubMed]
- Polsky, J.Y.; Garriguet, D. Change in vegetable and fruit consumption in Canada between 2004 and 2015. Health Rep. 2020, 31, 3–12. [Google Scholar] [PubMed]
- A Hu, E.; Pan, A.; Malik, V.; Sun, Q. White rice consumption and risk of type 2 diabetes: Meta-analysis and systematic review. BMJ 2012, 344, e1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Y.; Yang, X.; Xia, J.; Zhao, L.; Yang, Y. Consumption of meat and dairy products in China: A review. Proc. Nutr. Soc. 2016, 75, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Auclair, O.; Han, Y.; Burgos, S.A. Consumption of Milk and Alternatives and Their Contribution to Nutrient Intakes among Canadian Adults: Evidence from the 2015 Canadian Community Health Survey—Nutrition. Nutrients 2019, 11, 1948. [Google Scholar] [CrossRef] [Green Version]
- Government of Canada. What Are Canada’s Dietary Guidelines? Canada Food Guide; Health Canada: Ottawa, ON, Canada, 2020. Available online: https://food-guide.canada.ca/en/ (accessed on 20 May 2022).
- Government of Canada. Nutrients in Food; Health Canada: Ottawa, ON, Canada, 2015. Available online: https://www.canada.ca/en/health-canada/services/nutrients.html (accessed on 20 May 2022).
- Government of Canada. Fibre; Health Canada: Ottawa, ON, Canada, 2012. Available online: https://www.canada.ca/en/health-canada/services/nutrients/fibre.html (accessed on 20 May 2022).
- Yu, D.; Zhao, L.; Zhao, W. Status and trends in consumption of grains and dietary fiber among Chinese adults (1982–2015). Nutr. Rev. 2020, 78 (Suppl. 1), 43–53. [Google Scholar] [CrossRef]
- Worthy, L.D.; Lavigne, T.; Romero, F. Berry’s Model of Acculturation. In Culture and Psychology; Glendale Community College: Phoenix, AZ, USA, 2020. [Google Scholar]
- Aljaroudi, R.; Horton, S.; Hanning, R.M. Acculturation and Dietary Acculturation among Arab Muslim Immigrants in Canada. Can. J. Diet. Pract. Res. 2019, 80, 172–178. [Google Scholar] [CrossRef]
- Benazizi, I.; Ferrer-Serret, L.; Martínez-Martínez, J.M.; Ronda-Pérez, E.; Barbarà, C.I. Factors that influence the diet and eating habits of Chinese immigrant population in Catalonia (Spain). Gac. Sanit. 2021, 35, 12–20. [Google Scholar] [CrossRef]
- Popovic-Lipovac, A.; Strasser, B. A Review on Changes in Food Habits Among Immigrant Women and Implications for Health. J. Immigr. Minor. Health 2015, 17, 582–590. [Google Scholar] [CrossRef]
- Shi, L.; Zhang, D.; Rajbhandari-Thapa, J.; Katapodis, N.; Su, D.; Li, Y. Neighborhood immigrant density and population health among native-born Americans. Prev. Med. 2019, 127, 105792. [Google Scholar] [CrossRef]
- Lee, M.M.; Shen, J.M. Dietary patterns using Traditional Chinese Medicine principles in epidemiological studies. Asia Pac. J. Clin. Nutr. 2008, 17 (Suppl. 1), 79–81. [Google Scholar] [PubMed]
- Zhou, M.; Lee, R. Transnationalism and Community Building: Chinese Immigrant Organizations in the United States. ANNALS Am. Acad. Political Soc. Sci. 2013, 647, 22–49. [Google Scholar] [CrossRef]
- Valente, M.; Cortesi, P.A.; Lassandro, G.; Mathew, P.; Pocoski, J.; Molinari, A.C.; Mantovani, L.G.; Giordano, P. Health economic models in hemophilia A and utility assumptions from a clinician’s perspective. Pediatric Blood Cancer 2015, 62, 1826–1831. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Fahimi, S.; Singh, G.M.; Micha, R.; Khatibzadeh, S.; Engell, R.E.; Lim, S.; Danaei, G.; Ezzati, M.; Powles, J.; et al. Global Sodium Consumption and Death from Cardiovascular Causes. N. Engl. J. Med. 2014, 371, 624–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Wen, X.; Li, W.; Li, X.; Wang, Y.; Lu, W. Risk Factors for Stroke in the Chinese Population: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 509–517. [Google Scholar] [CrossRef]


{kind=link}
| Author Year | Research Setting | Research Design | Sampling | |
|---|---|---|---|---|
| 1 | Rodriguez et al. (2020) [19] | USA, community | Quantitative, cross-sectional secondary analysis from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) and the Multi-ethnic study of atherosclerosis (MESA), which were longitudinal studies | 3927 + 889 participants free of CVD |
| 2 | Beasley et al. (2019) [8] | New York City, USA | Quantitative, cross-sectional survey | 1973 Chinese immigrants, as part of Chinese American Cardiovascular Health Assessment |
| 3 | Chai et al. (2019) [20] | Delaware, USA, university setting | Quantitative cross-sectional survey | 172 Asian students, students, 108 from China or Taiwan |
| 4 | Kirshner et al. (2019) [21] | New York City, USA, community | Quantitative, cross-sectional survey | 2071 Chinese American New Yorkers, data from the Chinese American Cardiovascular Health Assessment |
| 5 | Higginbottom et al. (2018) [7] | Alberta, CAN, community | Quantitative, ethnography and interviews | 23 Chinese Canadian perinatal women |
| 6 | Zou (2018) [16] | Greater Toronto Area, CAN, telephone | Qualitative, telephone interviews | 30 aged Chinese-Canadian participants who received the DASHNa-CC |
| 7 | An (2017) [22] | United States, online | Quantitative, cross-sectional survey | 505 Chinese living in US, online |
| 8 | Liu et al. (2017) [23] | Greater Toronto Area, CAN, community | Mixed methods, qualitative focus group, and quantitative small-scale cross-sectional survey | 12 female Chinese immigrants, who had been in Canada for 10 years or less |
| 9 | Lu et al. (2017) [24] | Vancouver, Toronto, Halifax and St Catherines, CAN, community | Quantitative, cross-sectional survey | 100 Chinese immigrants aged 25+ |
| 10 | Wang et al. (2017) [23] | California, USA | Quantitative, cross-sectional | 2122 Asian adults, 658 of whom were Chinese |
| 11 | Zou (2017) [25] | Greater Toronto Area, CAN, classroom and community setting | Quantitative RCT, intervention received DASHNa-CC, control received usual care | 61 Chinese Canadians 45+ with hypertension but not on medications |
| 12 | Yi et al. (2016) [26] | New York City, USA, community | Quantitative, cross-sectional data obtained from New York City Community Health Survey | 555 Chinese America adults with hypertension, 144 South Asian adults with hypertension, 5987 Non Hispanic white adults with hypertension |
| 13 | Tseng et al. (2015) [27] | Philadelphia, USA, community | Quantitative, longitudinal study | 312 Chinese immigrant women |
| 14 | Corlin et al. (2014) [28] | Boston, USA, community-based | Quantitative, cross-sectional | 147 Chines immigrants and 167 US born whites participating in Community assessment of Freeway Exposure and Health study |
| 15 | Wyat et al. (2014) [29] | New York City, USA, community | Quantitative longitudinal, surveys over 4 years. | 805 Chinese Americans aged 65+, foreign-born |
| 16 | Adekunle et al. (2013) [30] | Greater Toronto Area, CAN | Quantitative, cross-sectional survey, predictive factor analysis | 250 Chinese Canadian respondents, representing household averaging four people |
| 17 | Wong et al. (2013) [31] | New York City, USA, community | Quantitative cross-sectional | 125 older (50+) Chinese persons |
| 18 | Tam et al. (2012) [32] | Toronto and Vancouver, CAN, community | Quantitative, Cross sectional | 1050 postmenopausal Canadian women, 421 of whom were recent Chinese migrants, 216 of whom migrated to the West before age 21 |
| 19 | Tseng et al. (2012) [33] | Philadelphia, USA, community | Quantitative, Cross-sectional surveys | 437 healthy premenopausal Chinese Immigrant women |
| 20 | Alonge et al. (2011) [34] | Houston, Texas, USA | Quantitative, Cross-sectional surveys | 213 Chinese, Mexican and Nigerian immigrants, 52 of whom were Chinese. |
| 21 | Lv et al. (2011) [35] | USA, community | Quantitative, Quasi-experimental study with a nested design and pre- and post design | 151 first generation Chinese American mothers between 35 and 55 |
| 22 | Rosenmoller et al. (2011) [36] | CAN, community | Quantitative, cross-sectional sub-study of the Multi-cultural Community health assessment Trial, study cohort | 120 Chinese-born people living in Canada |
| 23 | Tam et al. (2011) [37] | Toronto and Vancouver, CAN, community | Quantitative, cross-sectional | 1051 postmenopausal Canadian women, 383 of whom were recent Chinese migrants, 156 of whom migrated to the west before age 21 |
| 24 | Tseng et al. (2011) [38] | Philadelphia, USA, community | Quantitative cross-sectional surveys | 436 healthy premenopausal Chinese Immigrant women |
| 25 | Liu et al. (2010) [39] | Philadelphia, USA | Quantitative, cross-sectional | 243 Chinese Americans who were part of study on diet and breast density |
| 26 | Bell et al. (2009) [40] | British Columbia, CAN, professionally facilitated support group | Qualitative, ethnography | 96 Chinese Canadian participants in cancer support groups |
| 27 | Chesla et al. (2009) [41] | USA | Qualitative, comparative interview | 20 Chinese American couples, one with diabetes |
| 28 | Kwok et al. (2009) [42] | Toronto, CAN community | Quantitative, cross-sectional survey | 106 Chinese Canadians |
| 29 | Osypuk et al. (2009) [43] | Four USA cities, community | Quantitative, secondary analysis from the Multi-ethnic study of atherosclerosis, which was a longitudinal study | 1902 Study participants |
| 30 | Washington et al. (2009) [5] | California, USA, two Chinese senior care facilities | Qualitative semi-structured interviews | 13 participants, aged 65 years or older, who had a diagnosis of type 2 diabetes |
| 31 | Hislop (2008) [44] | Vancouver, CAN | Quantitative, cross-sectional | 504 Chinese adult immigrants |
| 32 | Kandula et al. (2008) [45] | USA: Baltimore, Chicago, Forsyth County, LA, NYC, St Paul | Cross-sectional data from Multi-Ethnic Study of Atherosclerosis | 1255 Hispanics and 737 Chinese participants |
| 33 | Lu et al. (2008) [46] | Western Canada, community | Qualitative, semi-structured interviews | 10 individuals |
| 34 | Taylor et al. (2007) [47] | Seattle, USA, community | Quantitative, cross-sectional survey | 495 Chinese immigrants |
| 35 | Babbar et al. (2006) [48] | New York City, USA, family care center | Mixed Methods, concurrent triangulation of cross-sectional study and qualitative surveys | 300 Chinese American Women |
| 36 | Fang et al. (2006) [49] | New York City, USA, hospital based | Quantitative, case control study | 187 foreign-born Chinese stroke cases and 204 controls matched |
| 37 | Walker et al. (2006) [50] | USA, community | Quantitative, development of prognostic model | 359 Chinese American women, ambulatory, ages 20–90 |
| 38 | Liang et al. (2004) [51] | Washington, DC, USA, community | Qualitative, focus groups | 54 Chinese American women aged 50+ |
| 39 | Lv et al. (2004) [52] | Pennsylvania, USA, community | Quantitative, cross-sectional self-administered survey | 399 Chinese Americans, 18+ in Pennsylvania |
| 40 | Lv et al. (2003) [53] | Pennsylvania, USA | Quantitative, cross-sectional survey | 399 Chinese Americans, 18+ in Pennsylvania |
| 41 | Kelemen et al. (2003) [54] | Hamilton, CAN, community | Quantitative, development of a tool (involved multiple 24 h recalls, items tabulated, assessed, and included into existing tool) | 74 immigrants, 25 of whom were Chinese |
| 42 | Satia-Abouta et al. (2002) [55] | Seattle, Vancouver, USA | Quantitative, Secondary analysis of data from Chinese Women’s Health Project, cross sectional | 244 adult females of Chinese ethnicity |
| 43 | Wu et al. (2002) [56] | Los Angeles County, USA | Quantitative case-control study | 523 cases, Asian American women between ages of 25–74 at time of diagnosis of breast cancer were identified through the LA Cancer Surveillance program. 160 were Chinese. 594 controls were selected from the neighbourhood. 228 were Chinese |
| 44 | Liou et al. (2001) [57] | New York City, USA, community | Quantitative, cross-sectional survey | 600 health Chinese Americans between 25 and 70 years of age |
| 45 | Satia et al. (2001) [58] | Seattle, USA and Vancouver, CAN community | Quantitative, Secondary analysis of data from Chinese Women’s Health Project, cross-sectional | 244 adult females of Chinese ethnicity |
| 46 | Satia et al. (2001) [59] | Seattle, USA, and Vancouver, CAN | Quantitative, Secondary analysis of data from Chinese Women’s Health Project, including cross-sectional survey, development of a measurement tool | 244 adult females of Chinese ethnicity |
| 47 | Satia et al. (2000) [60] | Seattle, USA, community | Qualitative interviews and focus groups, qualitative groundwork to develop quantitative dietary survey tool | 42 Chinese American women |
| 48 | Whittemore et al. (1995) [61] | USA: LA, San Francisco, Hawaii, CAN: Vancouver, Toronto In community and lab | Quantitative case control study | 1655 prostate cancer cases were identified through cancer registries in Hawaii, LA, SF, Vancouver, and Ontario Cancer Registry, 283 of whom were Chinese Americans. 1645 controls, 272 of whom were Chinese Americans |
| 49 | Choi et al. (1990) [62] | Boston, USA | Quantitative, cross-sectional surveys | 346 healthy elderly Chinese aged 60–96 |
| 50 | Whittemore et al. (1990) [63] | USA: LA, San Francisco, Vancouver CHINA: Hangzhou, Ningbo Hospitals | Quantitative, case-control study | 805 Chinese North American patients were identified from the British Columbia Cancer Registry |
| 51 | Newman et al. (1982) [64] | New York City, USA, community | Quantitative, cross-sectional surveys | 102 Chinese immigrant mothers |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, P.; Ba, D.; Luo, Y.; Yang, Y.; Zhang, C.; Zhang, H.; Wang, Y. Dietary Characteristics and Influencing Factors on Chinese Immigrants in Canada and the United States: A Scoping Review. Nutrients 2022, 14, 2166. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102166
Zou P, Ba D, Luo Y, Yang Y, Zhang C, Zhang H, Wang Y. Dietary Characteristics and Influencing Factors on Chinese Immigrants in Canada and the United States: A Scoping Review. Nutrients. 2022; 14(10):2166. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102166
Chicago/Turabian StyleZou, Ping, Dong Ba, Yan Luo, Yeqin Yang, Chunmei Zhang, Hui Zhang, and Yao Wang. 2022. "Dietary Characteristics and Influencing Factors on Chinese Immigrants in Canada and the United States: A Scoping Review" Nutrients 14, no. 10: 2166. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102166