
Effects of Omega-3 Supplementation Alone and Combined with Resistance Exercise on Skeletal Muscle in Older Adults: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
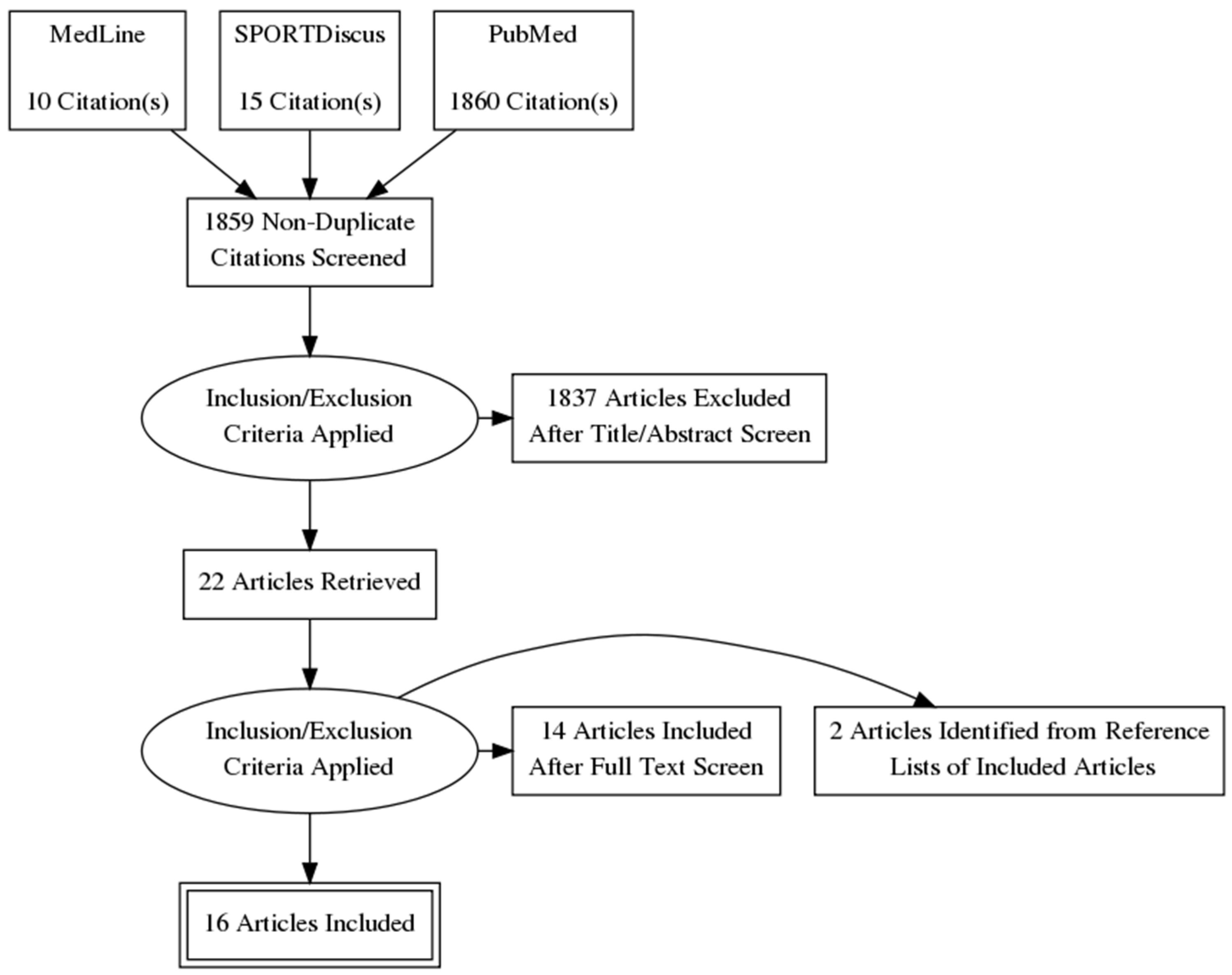
2. Materials and Methods
3. Results
3.1. Participant Characteristics
3.2. Intervention and Comparators
3.3. Risk of Bias
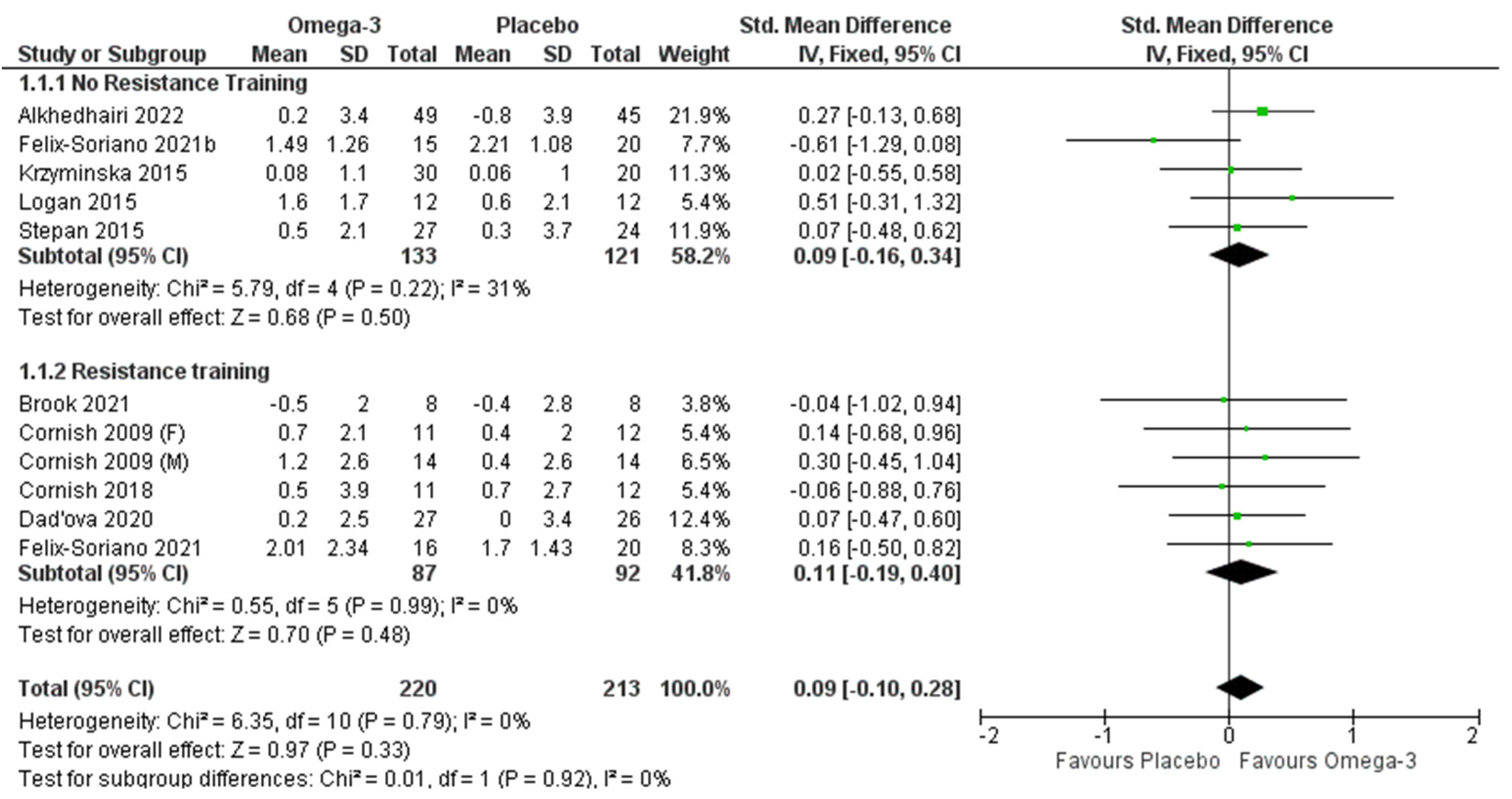
3.4. Lean Tissue Mass
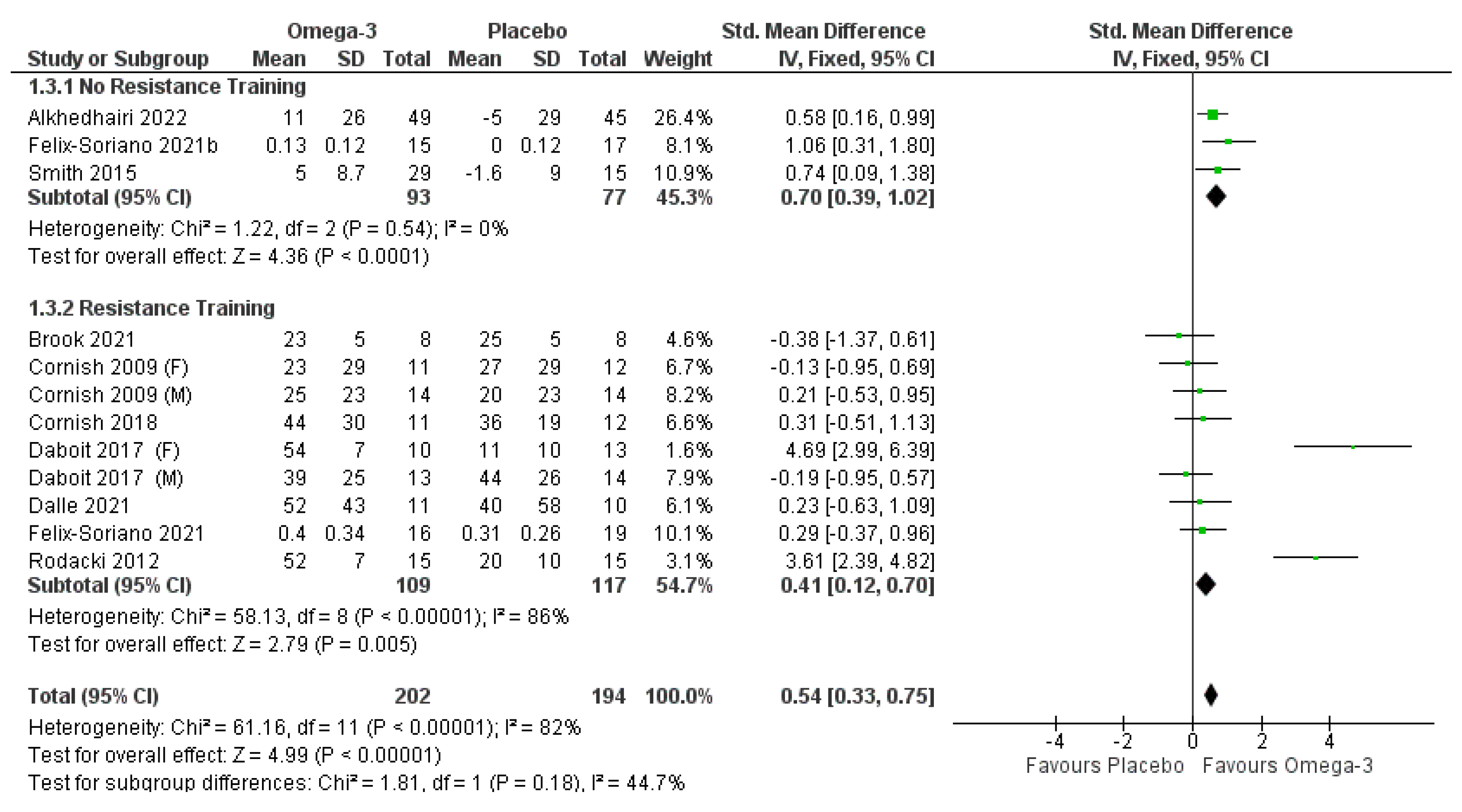
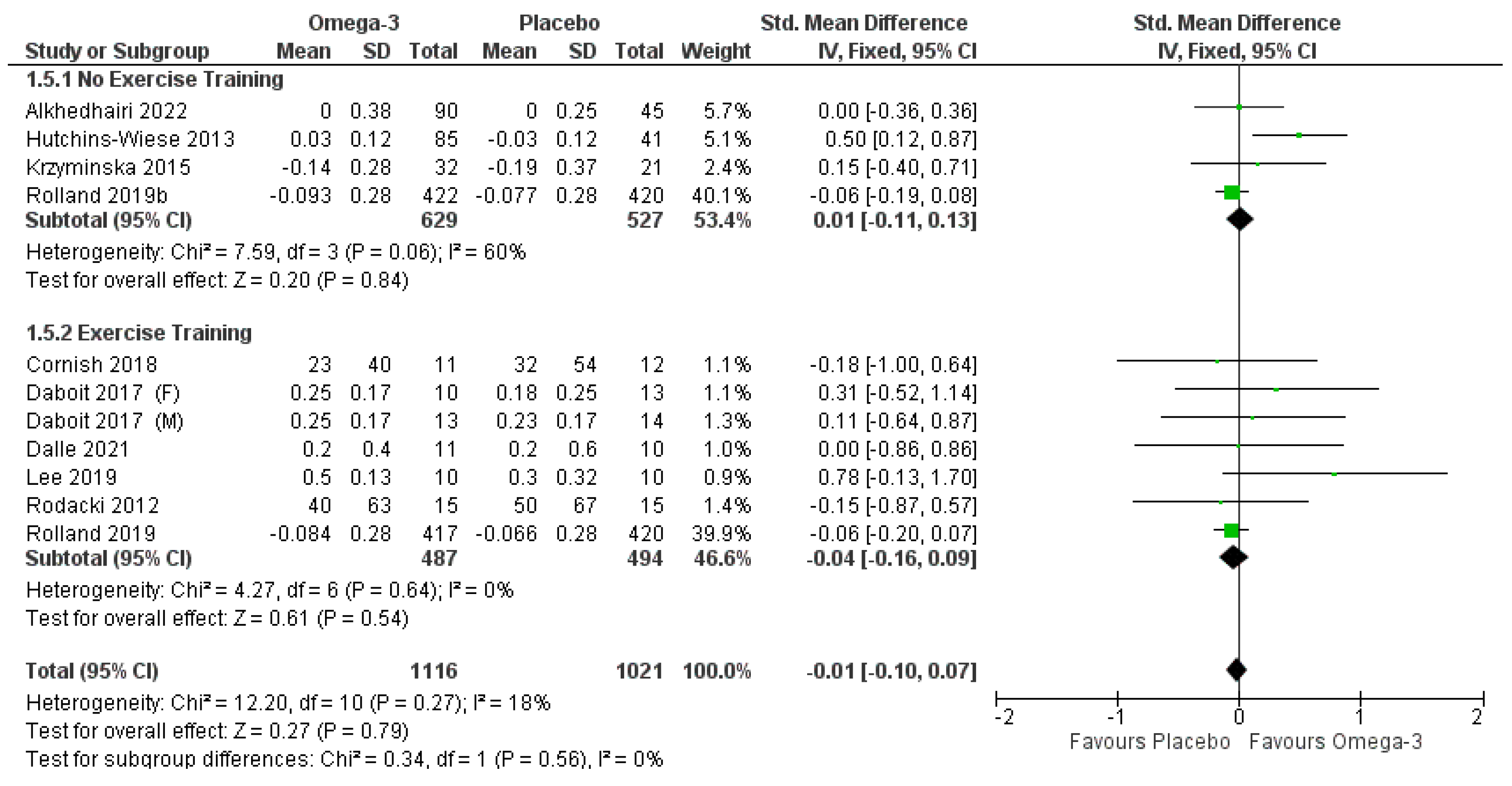
3.5. Lower Body Strength
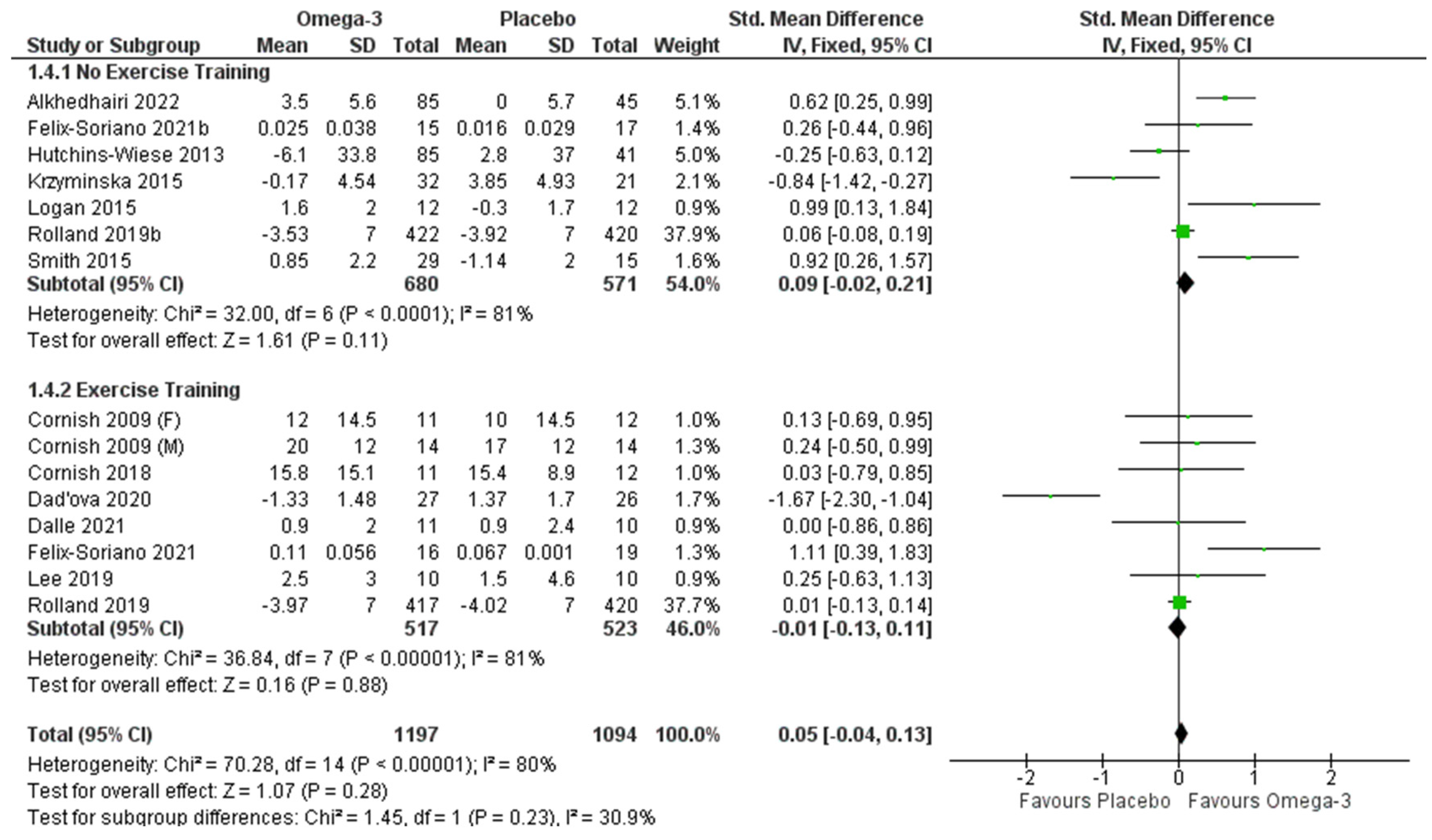
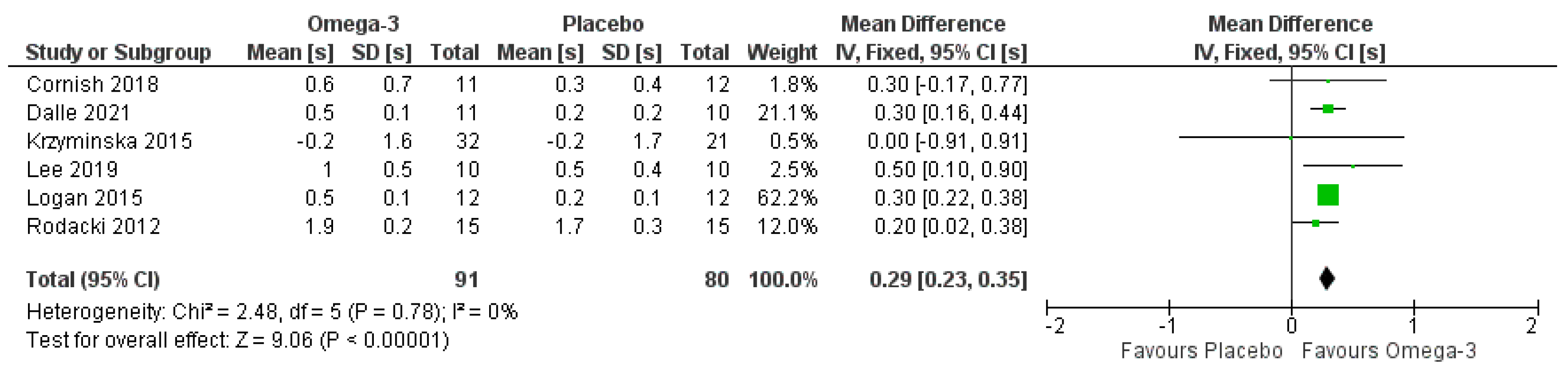
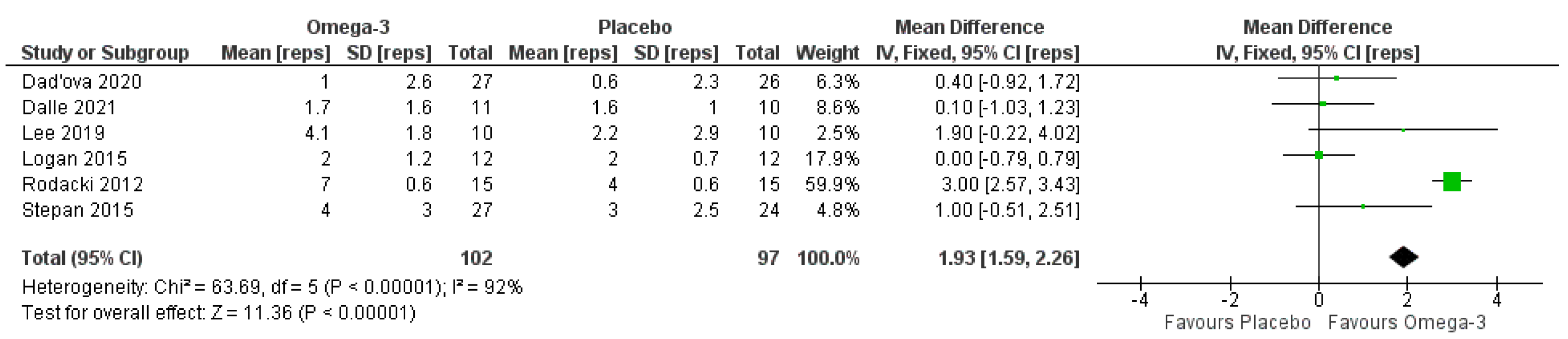
3.6. Functional Performance Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyère, O.; Beaudart, C.; Ethgen, O.; Reginster, J.-Y.; Locquet, M. The Health Economics Burden of Sarcopenia: A Systematic Review. Maturitas 2019, 119, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.-Y.; Shin, S. Sarcopenia Is Associated with Metabolic Syndrome in Korean Adults Aged over 50 Years: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1330. [Google Scholar] [CrossRef]
- Buchmann, N.; Fielitz, J.; Spira, D.; König, M.; Norman, K.; Pawelec, G.; Goldeck, D.; Demuth, I.; Steinhagen-Thiessen, E. Muscle Mass and Inflammation in Older Adults: Impact of the Metabolic Syndrome. Gerontology 2022, 1–10. [Google Scholar] [CrossRef]
- Nishikawa, H.; Asai, A.; Fukunishi, S.; Nishiguchi, S.; Higuchi, K. Metabolic Syndrome and Sarcopenia. Nutrients 2021, 13, 3519. [Google Scholar] [CrossRef]
- Kim, S.H.; Kang, H.W.; Jeong, J.B.; Lee, D.S.; Ahn, D.-W.; Kim, J.W.; Kim, B.G.; Lee, K.L.; Oh, S.; Yoon, S.H.; et al. Association of Obesity, Visceral Adiposity, and Sarcopenia with an Increased Risk of Metabolic Syndrome: A Retrospective Study. PLoS ONE 2021, 16, e0256083. [Google Scholar] [CrossRef]
- Park, H.-Y.; Jung, W.-S.; Kim, S.-W.; Lim, K. Relationship Between Sarcopenia, Obesity, Osteoporosis, and Cardiometabolic Health Conditions and Physical Activity Levels in Korean Older Adults. Front. Physiol. 2021, 12, 706259. [Google Scholar] [CrossRef]
- Wang, T. Searching for the Link between Inflammaging and Sarcopenia. Ageing Res. Rev. 2022, 77, 101611. [Google Scholar] [CrossRef]
- Rodrigues, F.; Domingos, C.; Monteiro, D.; Morouço, P. A Review on Aging, Sarcopenia, Falls, and Resistance Training in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 874. [Google Scholar] [CrossRef]
- Fyfe, J.J.; Hamilton, D.L.; Daly, R.M. Minimal-Dose Resistance Training for Improving Muscle Mass, Strength, and Function: A Narrative Review of Current Evidence and Practical Considerations. Sports Med. 2022, 52, 463–479. [Google Scholar] [CrossRef] [PubMed]
- Mende, E.; Moeinnia, N.; Schaller, N.; Weiß, M.; Haller, B.; Halle, M.; Siegrist, M. Progressive Machine-Based Resistance Training for Prevention and Treatment of Sarcopenia in the Oldest Old: A Systematic Review and Meta-Analysis. Exp. Gerontol. 2022, 163, 111767. [Google Scholar] [CrossRef] [PubMed]
- Tsekoura, M.; Billis, E.; Kastrinis, A.; Katsoulaki, M.; Fousekis, K.; Tsepis, E.; Konstantoudaki, X.; Gliatis, J. The Effects of Exercise in Patients with Sarcopenia. Adv. Exp. Med. Biol. 2021, 1337, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Yuen, Y. Effects of Resistance Training on C-Reactive Protein and Inflammatory Cytokines in Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 3434. [Google Scholar] [CrossRef]
- Vikberg, S.; Sörlén, N.; Brandén, L.; Johansson, J.; Nordström, A.; Hult, A.; Nordström, P. Effects of Resistance Training on Functional Strength and Muscle Mass in 70-Year-Old Individuals with Pre-Sarcopenia: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2019, 20, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Giallauria, F.; Cittadini, A.; Smart, N.A.; Vigorito, C. Resistance Training and Sarcopenia. Monaldi Arch. Chest Dis. Arch. Monaldi Mal. Torace 2016, 84, 738. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, E.J.; Seigel, J.W.; McGlory, C. Omega-3 Fatty Acids and Human Skeletal Muscle. Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 114–119. [Google Scholar] [CrossRef]
- Jang, I.-Y.; Jung, H.-W.; Park, J.H.; Kim, J.H.; Lee, S.; Lee, E.; Lee, J.Y.; Park, S.J.; Kim, D.A.; Kim, S.J.; et al. Lower Serum N-3 Fatty Acid Level in Older Adults with Sarcopenia. Nutrients 2020, 12, 2959. [Google Scholar] [CrossRef]
- Calder, P.; Grimble, R. Polyunsaturated Fatty Acids, Inflammation and Immunity. Eur. J. Clin. Nutr. 2002, 56, S14–S19. [Google Scholar] [CrossRef] [Green Version]
- James, M.J.; Gibson, R.A.; Cleland, L.G. Dietary Polyunsaturated Fatty Acids and Inflammatory Mediator Production. Am. J. Clin. Nutr. 2000, 71, 343s–348s. [Google Scholar] [CrossRef]
- Candow, D.G.; Forbes, S.C.; Little, J.P.; Cornish, S.M.; Pinkoski, C.; Chilibeck, P.D. Effect of Nutritional Interventions and Resistance Exercise on Aging Muscle Mass and Strength. Biogerontology 2012, 13, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Bird, J.K.; Troesch, B.; Warnke, I.; Calder, P.C. The Effect of Long Chain Omega-3 Polyunsaturated Fatty Acids on Muscle Mass and Function in Sarcopenia: A Scoping Systematic Review and Meta-Analysis. Clin. Nutr. ESPEN 2021, 46, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-H.; Chiu, W.-C.; Hsu, Y.-P.; Lo, Y.-L.; Wang, Y.-H. Effects of Omega-3 Fatty Acids on Muscle Mass, Muscle Strength and Muscle Performance among the Elderly: A Meta-Analysis. Nutrients 2020, 12, 3739. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.N.; Watt, A.E.; Isenring, E.A.; de van der Schueren, M.A.E.; van der Meij, B.S. The Effect of Oral Omega-3 Polyunsaturated Fatty Acid Supplementation on Muscle Maintenance and Quality of Life in Patients with Cancer: A Systematic Review and Meta-Analysis. Clin. Nutr. 2021, 40, 3815–3826. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Cornish, S.M.; Chilibeck, P.D. Alpha-Linolenic Acid Supplementation and Resistance Training in Older Adults. Appl. Physiol. Nutr. Metab. 2009, 34, 49–59. [Google Scholar] [CrossRef]
- Lee, S.-R.; Jo, E.; Khamoui, A.V. Chronic Fish Oil Consumption with Resistance Training Improves Grip Strength, Physical Function, and Blood Pressure in Community-Dwelling Older Adults. Sports 2019, 7, 167. [Google Scholar] [CrossRef] [Green Version]
- Daďová, K.; Petr, M.; Šteffl, M.; Sontáková, L.; Chlumský, M.; Matouš, M.; Štich, V.; Štěpán, M.; Šiklová, M. Effect of Calanus Oil Supplementation and 16 Week Exercise Program on Selected Fitness Parameters in Older Women. Nutrients 2020, 12, 481. [Google Scholar] [CrossRef] [Green Version]
- Rolland, Y.; de Barreto, P.S.; Maltais, M.; Guyonnet, S.; Cantet, C.; Andrieu, S.; Vellas, B. Effect of Long-Term Omega 3 Polyunsaturated Fatty Acid Supplementation with or without Multidomain Lifestyle Intervention on Muscle Strength in Older Adults: Secondary Analysis of the Multidomain Alzheimer Preventive Trial (MAPT). Nutrients 2019, 11, 1931. [Google Scholar] [CrossRef] [Green Version]
- Félix-Soriano, E.; Martínez-Gayo, A.; Cobo, M.J.; Pérez-Chávez, A.; Ibáñez-Santos, J.; Palacios Samper, N.; Goikoetxea Galarza, I.; Cuervo, M.; García-Unciti, M.; González-Muniesa, P.; et al. Effects of DHA-Rich n-3 Fatty Acid Supplementation and/or Resistance Training on Body Composition and Cardiometabolic Biomarkers in Overweight and Obese Post-Menopausal Women. Nutrients 2021, 13, 2465. [Google Scholar] [CrossRef] [PubMed]
- Štěpán, M.; Daďová, K.; Matouš, M.; Krauzová, E.; Sontáková, L.; Koc, M.; Larsen, T.; Kuda, O.; Štich, V.; Rossmeislová, L.; et al. Exercise Training Combined with Calanus Oil Supplementation Improves the Central Cardiodynamic Function in Older Women. Nutrients 2021, 14, 149. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Julliand, S.; Reeds, D.N.; Sinacore, D.R.; Klein, S.; Mittendorfer, B. Fish Oil-Derived n-3 PUFA Therapy Increases Muscle Mass and Function in Healthy Older Adults. Am. J. Clin. Nutr. 2015, 102, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, S.L.; Spriet, L.L. Omega-3 Fatty Acid Supplementation for 12 Weeks Increases Resting and Exercise Metabolic Rate in Healthy Community-Dwelling Older Females. PLoS ONE 2015, 10, e0144828. [Google Scholar] [CrossRef]
- Brook, M.S.; Din, U.; Tarum, J.; Selby, A.; Quinlan, J.; Bass, J.J.; Gharahdaghi, N.; Boereboom, C.; Abdulla, H.; Franchi, M.V.; et al. Omega-3 Supplementation during Unilateral Resistance Exercise Training in Older Women: A within Subject and Double-Blind Placebo-Controlled Trial. Clin. Nutr. ESPEN 2021, 46, 394–404. [Google Scholar] [CrossRef]
- Dalle, S.; Van Roie, E.; Hiroux, C.; Vanmunster, M.; Coudyzer, W.; Suhr, F.; Bogaerts, S.; Van Thienen, R.; Koppo, K. Omega-3 Supplementation Improves Isometric Strength but Not Muscle Anabolic and Catabolic Signaling in Response to Resistance Exercise in Healthy Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 406–414. [Google Scholar] [CrossRef]
- Cornish, S.M.; Myrie, S.B.; Bugera, E.M.; Chase, J.E.; Turczyn, D.; Pinder, M. Omega-3 Supplementation with Resistance Training Does Not Improve Body Composition or Lower Biomarkers of Inflammation More so than Resistance Training Alone in Older Men. Nutr. Res. 2018, 60, 87–95. [Google Scholar] [CrossRef]
- Da Boit, M.; Sibson, R.; Sivasubramaniam, S.; Meakin, J.R.; Greig, C.A.; Aspden, R.M.; Thies, F.; Jeromson, S.; Hamilton, D.L.; Speakman, J.R.; et al. Sex Differences in the Effect of Fish-Oil Supplementation on the Adaptive Response to Resistance Exercise Training in Older People: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2017, 105, 151–158. [Google Scholar] [CrossRef]
- Krzymińska-Siemaszko, R.; Czepulis, N.; Lewandowicz, M.; Zasadzka, E.; Suwalska, A.; Witowski, J.; Wieczorowska-Tobis, K. The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass. Int. J. Environ. Res. Public Health 2015, 12, 10558–10574. [Google Scholar] [CrossRef] [Green Version]
- Alkhedhairi, S.A.; Aba Alkhayl, F.F.; Ismail, A.D.; Rozendaal, A.; German, M.; MacLean, B.; Johnston, L.; Miller, A.A.; Hunter, A.M.; Macgregor, L.J.; et al. The Effect of Krill Oil Supplementation on Skeletal Muscle Function and Size in Older Adults: A Randomised Controlled Trial. Clin. Nutr. 2022, 41, 1228–1235. [Google Scholar] [CrossRef]
- Hutchins-Wiese, H.L.; Kleppinger, A.; Annis, K.; Liva, E.; Lammi-Keefe, C.J.; Durham, H.A.; Kenny, A.M. The Impact of Supplemental N-3 Long Chain Polyunsaturated Fatty Acids and Dietary Antioxidants on Physical Performance in Postmenopausal Women. J. Nutr. Health Aging 2013, 17, 76–80. [Google Scholar] [CrossRef]
- Rodacki, C.L.N.; Rodacki, A.L.F.; Pereira, G.; Naliwaiko, K.; Coelho, I.; Pequito, D.; Fernandes, L.C. Fish-Oil Supplementation Enhances the Effects of Strength Training in Elderly Women. Am. J. Clin. Nutr. 2012, 95, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Chilibeck, P.D. Differences in Size, Strength, and Power of Upper and Lower Body Muscle Groups in Young and Older Men. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 148–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Crouch, R. 1-Minute Sit-to-Stand Test: Systematic Review of Procedures, Performance, and Clinimetric Properties. J. Cardiopulm. Rehabil. Prev. 2019, 39, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Pangilinan, J.; Quanstrom, K.; Bridge, M.; Walter, L.C.; Finlayson, E.; Suskind, A.M. The Timed Up and Go Test as a Measure of Frailty in Urologic Practice. Urology 2017, 106, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Park, C.; Sharafkhaneh, A.; Bryant, M.S.; Nguyen, C.; Torres, I.; Najafi, B. Toward Remote Assessment of Physical Frailty Using Sensor-Based Sit-to-Stand Test. J. Surg. Res. 2021, 263, 130–139. [Google Scholar] [CrossRef] [PubMed]
- McGlory, C.; Calder, P.C.; Nunes, E.A. The Influence of Omega-3 Fatty Acids on Skeletal Muscle Protein Turnover in Health, Disuse, and Disease. Front. Nutr. 2019, 6, 144. [Google Scholar] [CrossRef] [Green Version]
- Gray, S.R.; Mittendorfer, B. Fish Oil-Derived n-3 Polyunsaturated Fatty Acids for the Prevention and Treatment of Sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Di Girolamo, F.G.; Situlin, R.; Mazzucco, S.; Valentini, R.; Toigo, G.; Biolo, G. Omega-3 Fatty Acids and Protein Metabolism: Enhancement of Anabolic Interventions for Sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 145–150. [Google Scholar] [CrossRef]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Dietary Omega-3 Fatty Acid Supplementation Increases the Rate of Muscle Protein Synthesis in Older Adults: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2011, 93, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Bazan, N.G.; Molina, M.F.; Gordon, W.C. Docosahexaenoic Acid Signalolipidomics in Nutrition: Significance in Aging, Neuroinflammation, Macular Degeneration, Alzheimer’s, and Other Neurodegenerative Diseases. Annu. Rev. Nutr. 2011, 31, 321–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, N.; He, X.; Feng, Y.; Ainsworth, B.E.; Liu, Y. Effects of Resistance Training in Healthy Older People with Sarcopenia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Rev. Aging Phys. Act. 2021, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Beckwée, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I. Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Talar, K.; Hernández-Belmonte, A.; Vetrovsky, T.; Steffl, M.; Kałamacka, E.; Courel-Ibáñez, J. Benefits of Resistance Training in Early and Late Stages of Frailty and Sarcopenia: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. J. Clin. Med. 2021, 10, 1630. [Google Scholar] [CrossRef] [PubMed]
- Watt, J.; Colley, R. Youth—But Not Adults—Reported Less Physical Activity during the COVID-19 Pandemic. Available online: https://www150.statcan.gc.ca/n1/en/catalogue/45280001202100100032 (accessed on 10 April 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Design | Sample | Intervention | Main Results |
|---|---|---|---|---|
| No RET | ||||
| Alkhedhairi et al. [40] | Double-blind RCT | n = 94; female, n = 53; male, n = 41; age = 71.2 ± 5.1 years | Krill oil (4 g/day; 772 mg/d EPA and 384 mg/day DHA) or placebo (4 g/day mixed vegetable oil) for 6 months | Krill oil supplementation resulted in improved knee extensor maximal torque (9.3%), grip strength (10.9%), and vastus lateralis muscle thickness (3.5%) to a greater extent than placebo. However, there was no difference in short performance physical battery test between groups. |
| Hutchins-Wiese et al. [41] | Double-blind RCT | n = 126; all female; age, 75 (range 64–95) years | ω-3 (1.2 g/day EPA and 1.2 g/day DHA) or placebo (1.8 g/day olive oil) | Higher RBC DHA content and DHA/AA ratio was associated with less frailty (p = 0.007 and p = 0.004, respectively). Fish oil supplementation improved walking speed compared to placebo (p = 0.038). |
| Krzymińska-Siemaszko et al. [39] | Non-blinded RCT | n = 50; 17 male and 33 female; age, 74.6 ± 8.0 years; all with decreased muscle mass | ω-3 (1.3 g/day PUFA (2 capsules/day containing 600 mg EPA, 440 DHA, 200 mg other ω-3 fatty acids) and 10 mg/day vitamin E) or placebo (11 mg/day vitamin E solution) for 12 weeks | No difference in muscle mass, grip strength, timed-up-and-go test, or appendicular lean mass index. |
| Logan and Spriet [34] | Single-blind RCT | n = 24; all female; age = 66 ± 1 years | ω-3 (5 g/day (2 g/day EPA and 1 g/day DHA)) or placebo (3 g/day olive oil) for 12 weeks | ω-3 supplementation resulted in increased lean mass (4%) and timed-up-and-go test (7%), while no improvements were observed in the placebo group. No improvements were observed in grip strength or 30-s sit-to-stand test for either group. |
| Rolland et al. [30] | Double-blind RCT | n = 1679; age = 75.34 ± 4.42 years | ω-3 (800 mg/day DHA and 225 mg/day EPA), placebo (paraffin oil), ω-3 and a multidomain intervention (including physical activity and nutrition advice, and cognitive training), or placebo and multidomain intervention for 36 months | No differences between groups were found for chair-stand test, handgrip strength, 4-m walking speed, or short physical performance battery. |
| Smith et al. [33] | Double-blind RCT | n = 44; male = 15 and female = 29; age, control = 69.7 ± 7 years and omega-3 = 68 ± 5 years (mean ± SEM) | ω-3 (4 × 1 g pills/day providing 1.86 g/day EPA and 1.5 g/day DHA) or placebo (4 × 1 g pills/day of corn oil) for 6 months | ω-3 supplementation increased thigh muscle volume, handgrip strength, and 1 repetition maximum muscle strength compared to control. Average isokinetic power approached significance with ω-3 supplementation as well (p = 0.075). |
| With RET | ||||
| Brook et al. [35] | Double-blind RCT | n = 16; female; age, placebo = 66.5 ± 1.4 years and ω-3 = 64.4 ± 0.8 years | ω-3 PUFA (3680 mg/day (1860 mg EPA and 1540 mg DHA)) or placebo (corn oil) for 6 weeks | 1 repetition maximum and number of myonuclei in type I and type II fibres increased equally in treatment arms. ω-3 supplementation resulted in greater thigh fat free mass and type II fibre cross sectional area, as well as greater 4EBP1 activation after acute RE at the 6-week time-point compared to placebo. No differences in maximum voluntary contraction, type I fibre cross sectional area, and satellite cell number were observed between groups. |
| Cornish and Chilibeck [27] | Double-blind RCT | n = 51; age, 65.4 ± 0.8 years; male = 28, female = 23 | Flaxseed oil 30 mL/day (~14 g/day ALA) or placebo (30 mL/day corn oil) for 12 weeks | Males supplementing with ALA demonstrated decreased systemic IL-6 concentrations and increased knee flexor muscle thickness following 12 weeks of RET. Females demonstrated no additional benefit associated with ALA supplementation. |
| Cornish et al. [37] | Pilot double-blind RCT | n = 23; all male; age, ω-3 = 71.4 ± 6.2 years and placebo = 70.9 ± 5.0 years | 3.0 g/day ω-3 (1.98 g EPA and 0.99 g DHA) or placebo (ω 3-6-9 blend, 1350 mg ALA, 795 mg linoleic acid and γ-linolenic acid, 525 mg oleic acid, 330 mg of other short-chain fatty acids, saturated fat, and phospholipids) for 12 weeks | RET improved lean tissue mass, chest press and leg press strength, and physical function, with no added benefits with ω-3 supplementation. |
| Da Boit et al. [38] | Double-blind RCT | n = 50; male: n = 27 and female: n = 23; age, male = 70.6 ± 4.5 years and female = 70.7 ± 3.3 years | ω-3 (3.0 g/day fish oil) or placebo (3 g/day safflower oil) for 18 weeks | In females supplemented with ω-3 fatty acids, maximal isometric torque and muscle quality improved to a greater extent than placebo, with no difference in males. |
| Daďová et al. [29] | Double-blind RCT | n = 55; all female; age = 70.9 ± 3.9 years | Calanus oil (~105 mg/day DHA and 125 mg/day EPA) or placebo (sunflower oil) and combined aerobic and RET training for 16 weeks | Calanus oil improved chair-stand test repetitions (calanus oil, median ∆ = 4 vs. placebo median ∆ = 3) but not muscle mass compared to placebo. |
| Dalle et al. [36] | Double-blind RCT | n = 23; male: n = 8 and female: n = 15; age range, 65–84 years | ω-3 (1100 mg three times/day (410 mg DHA, 540 mg EPA and 4 mg vitamin E) or placebo (1100 mg corn oil three times/day) for 14 weeks | ω-3 supplementation enhanced isometric strength gains but not muscle volume, catabolic, or inflammatory adaptations in response to RET. |
| Félix-Soriano et al. [31] | Double-blind RCT | n = 67; all overweight/obese females; age range, 55–70 years | Placebo (3 g/day olive oil), ω-3 (3 g/day containing 1650 mg DHA and 150 mg EPA), placebo and RET, omega-3 and RET for 16 weeks | RET resulted in improved upper limb lean mass, muscle strength, and muscle quality compared to the untrained groups. ω-3 supplementation improved muscle quality of the lower limbs. |
| Lee et al. [28] | RCT | n = 28; 10 males and 18 females; age, 66.5 ± 5.0 years | ω-3 (2.1 g/day EPA and 0.72 g/day EHA) and RT, placebo (safflower oil) and RET, and control only for 12 weeks | RET resulted in improved handgrip strength, five times sit-to-stand, timed-up-and-go, 6-m walk, and 30-s sit-to-stand. |
| Rodacki et al. [42] | Randomized, non-controlled | n = 45; all female; age = 64 ± 1.4 years | All completed 90 RET. One group only did RET; another consumed fish oil during RET; lastly, a group consumed fish oil for 60 days prior to RET. Participants receiving fish oil consumed 2 g/day (~0.4 g/d EPA and 0.3 g/day DHA) | Both groups that consumed fish oil had greater improvements in peak torque and rate of torque development and chair-rising performance compared to the RET only group. |
| Štěpán et al. [32] | Double-blind RCT | n = 55; all female; placebo, age = 70 ± 4 years; Calanus oil, age = 71 ± 4 years | Calanus oil (~230 mg/day EPA + DHA) or placebo (sunflower oil) combined aerobic and RET for 4 months | Exercise training resulted in improved lean body mass, arm curl repetitions, and chair-stand test for both groups. Additionally, an interaction effect was identified for chair-stand test (mean ∆, calanus oil = 4 vs. placebo = 3), indicating calamus oil supplementation may contribute to greater improvements. |
| Study | Risk of Bias Domain | ||||||
|---|---|---|---|---|---|---|---|
| Randomization Process | Period or Carry-Over Effect | Deviation from Intended Intervention | Missing Outcome Data | Measurement of Outcome | Selection of Reported Results | Overall Risk of Bias | |
| Alkhedhairi et al. [40] | Low | Low | Low | Low | Low | Low | Low |
| Hutchins-Wiese et al. [41] | Low | Low | Low | Low | Low | Low | Low |
| Krzymińska-Siemaszko et al. [39] | Low | Low | Low | Low | High | Some Concerns | High |
| Logan and Spriet [34] | Low | Low | Low | Low | High | Some Concerns | High |
| Rolland et al. [30] | Low | Low | Low | Low | Low | Low | Low |
| Smith et al. [33] | Low | Low | Low | Low | Low | Low | Low |
| Brook et al. [35] | Low | Low | Low | Low | Low | Low | Low |
| Cornish and Chilibeck [27] | Low | Low | Low | Low | Low | Some Concerns | Some Concerns |
| Cornish et al. [37] | Low | Low | Low | Low | Low | Some Concerns | Some Concerns |
| Da Boit et al. [38] | Low | Low | Low | Low | Low | Low | Low |
| Daďová et al. [29] | Low | Low | Low | Low | Low | Low | Low |
| Dalle et al. [36] | Low | Low | Low | Low | Low | Low | Low |
| Félix-Soriano et al. [31] | Low | Low | Low | Low | Low | Low | Low |
| Lee et al. [28] | Low | Low | Low | Low | Low | Some Concerns | Some Concerns |
| Rodacki et al. [42] | Low | Low | Low | Low | High | Some Concerns | High |
| Štěpán et al. [32] | Low | Low | Low | Low | Low | Low | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cornish, S.M.; Cordingley, D.M.; Shaw, K.A.; Forbes, S.C.; Leonhardt, T.; Bristol, A.; Candow, D.G.; Chilibeck, P.D. Effects of Omega-3 Supplementation Alone and Combined with Resistance Exercise on Skeletal Muscle in Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2221. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112221
Cornish SM, Cordingley DM, Shaw KA, Forbes SC, Leonhardt T, Bristol A, Candow DG, Chilibeck PD. Effects of Omega-3 Supplementation Alone and Combined with Resistance Exercise on Skeletal Muscle in Older Adults: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(11):2221. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112221
Chicago/Turabian StyleCornish, Stephen M., Dean M. Cordingley, Keely A. Shaw, Scott C. Forbes, Taylor Leonhardt, Ainsley Bristol, Darren G. Candow, and Philip D. Chilibeck. 2022. "Effects of Omega-3 Supplementation Alone and Combined with Resistance Exercise on Skeletal Muscle in Older Adults: A Systematic Review and Meta-Analysis" Nutrients 14, no. 11: 2221. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112221