1. Introduction
Skin cancer represents the most frequent type of cancer in the Caucasian population.
Non-melanoma skin cancers (NMSCs) are widely spread, with increasing incidence and represent a pleomorphic group, both clinically and histologically, compared to malignant melanoma (MM) where using the classical evaluation of ABCDE, a correct diagnosis can be made 97% of the time, solely by clinical means.
NMSCs comprise all the non-melanoma malignant skin tumors, of which 99% are represented by keratinocyte carcinomas, namely basal (BCC) and squamous cell carcinoma (SCC) [
1].
NMSCs constitute the largest group tumors addressed by plastic surgeons, either for excision or for reconstructive purposes. NMSCs consist of basal cell carcinoma (BCC), cutaneous squamous cell carcinoma (CSCC) and Bowen’s disease. The high number of NMSC cases pose economic questions regarding spending and loss. Age, gender, ultraviolet light, fair skin, ionizing radiation, immunosuppression, previous skin cancer or premalignant lesions are common associated risk factors.
Facial tumors are the most commonly addressed localization of tumors in patients treated by plastic surgeons, with Non-melanoma skin cancer (NMSCs) representing 99% of all presented cases. The incidence of both MM and NMSC is on the rise, with annual increase in MM of 0.6% among adults over 50 years [
2]. In this present study, due to the high incidence of facial NMSC compared to MM and the miscorrelation between clinical diagnostics and histopathology, we evaluated and tried to define a series of clinical criteria for NMSC diagnostics and the correlations with the pathology exams.
BCC, the most prevalent type of NMSC, is located with predilection on the nose and can be addressed by incisional biopsy. Treating BCC can be fulfilled by non-excisional or excisional means, the choice of treatment being dependent on the risk factors.
CSCC is the second most frequent NMSC and aside from BCC, it can metastasize to the regional lymph nodes. Burn wounds and chronic non-healing wounds can transform into CSCC. Treatment is based on the pathological report [
3].
Finding a correlation between clinical aspects, risk factor parameters and type of tumor confirmed by pathology can aid in correct diagnostic, proper excision limits and early reconstruction of post-excisional facial defects.
2. Materials and Methods
A descriptive retrospective study was done, including patients with facial tumors who attended the Plastic and Reconstructive Clinic and the Otorhinolaryngology Clinic from the “Sf. Spiridon” Emergency Hospital from Iași, Romania for diagnosis and surgical treatment, during a period of 3 years: January 2015–December 2017. The study was approved by the Ethics Commission of University of Medicine and Pharmacy “Grigore T. Popa” Iasi, 1 May 2018 in compliance with ethical and deontological rules for medical and research practice.
The total number of cases included in the study was 186, from which 81 had been clinically associated with benign tumors, 70 with BCC and 35 with squamous cell carcinomas (SCC).
The 81 cases with benign pathology (35 males and 46 females) were associated with 109 tumors.
As stated above, 70 cases were associated with BCC (31 males and 39 females) and corresponded with a total of 82 tumors. From these patients, 54 were above 60 years of age and 26 were below 60. The youngest patient was 26 years old with an associated upper eyelid BCC.
The 35 cases with SCC were divided into 12 males and 23 females.
3. Results
3.1. Benign Tumors
As mentioned before, 81 cases had benign pathology, totaling 109 tumors; this leads to the conclusion that multiple tumors were associated with one case. The maximum number of performed excisions per case was seven.
Multiple types of benign tumors were encountered. The permanent challenge was to state an accurate initial clinical diagnosis; the success rate of this was confirmed by the results of the histological examinations. However, there have been cases in which the clinical diagnosis was confirmed by the laboratory. We described the various types of benign tumors and the correspondence between the clinical and the histological diagnosis.
From a total of 36 clinically diagnosed skin nevi, the anatomopathological exam revealed 13 different histological diagnoses: one hemangioma, two papilloma’s and 10 cases of keratosis. From eight lipomas, three were not confirmed by the laboratory. Sixteen sebaceous cysts were clinically diagnosed, from which six had a different result. From six hemangiomas, two were later described as a BCC of the orbital region. Four cases of teratomas were confirmed.
From nine presumed warts, four were discovered to be skin nevi. Eleven tumors were initially described as keratoacanthomas, of which two were confirmed as skin nevi. In one case, the suspicion of glomangioma was confirmed by the histological diagnosis of hemangioma. Glomus tumors represent 1–5% of soft tissue tumors of the hand and 75% are in a subungual location. Glomus tumors usually present as bluish or pinkish red. The clinical triad of tenderness, severe pain and cold sensitivity, along with the cold sensitivity test were reported to be reliable for diagnosis [
4].
Ten squamous cell papillomas were suspected; two were confirmed as basal cell carcinomas and three as skin nevi. From 12 presumed basal cell papillomas (seborrheic keratosis), seven were described as skin nevi. All of the four suspected actinic keratosis were described by the histological exam as BCC. One suspicion of hidradenoma was described by the laboratory as hemangioma.
To summarize, 57 initial clinical diagnoses matched the histological findings and 52 had different anatomopathological diagnoses.
Looking at things from a different perspective, from the 109 histologically confirmed benign facial skin tumors, 99 were initially suspected of being benign and 10 had a clinical diagnosis of malign tumors which was confirmed by the histological results (nine suspected BCC and one SCC that was later described as pilomatrixoma).
However, we also describe the initial clinical diagnoses of benign tumors that after extensive histological examination were found to be of malignant nature or the other way around; we will further describe some of these circumstances.
A case of a suspected upper eyelid sebaceous cyst was histologically described as a rare sebaceous carcinoma. Sebaceous carcinoma is a rare malignant tumor often localized in the periorbital area, and is also called adenocarcinoma of the sebaceous gland, Meibomian gland carcinoma, or Zeiss gland carcinoma. The tumor is locally aggressive and can metastasize to regional lymph nodes and distant organs [
5].
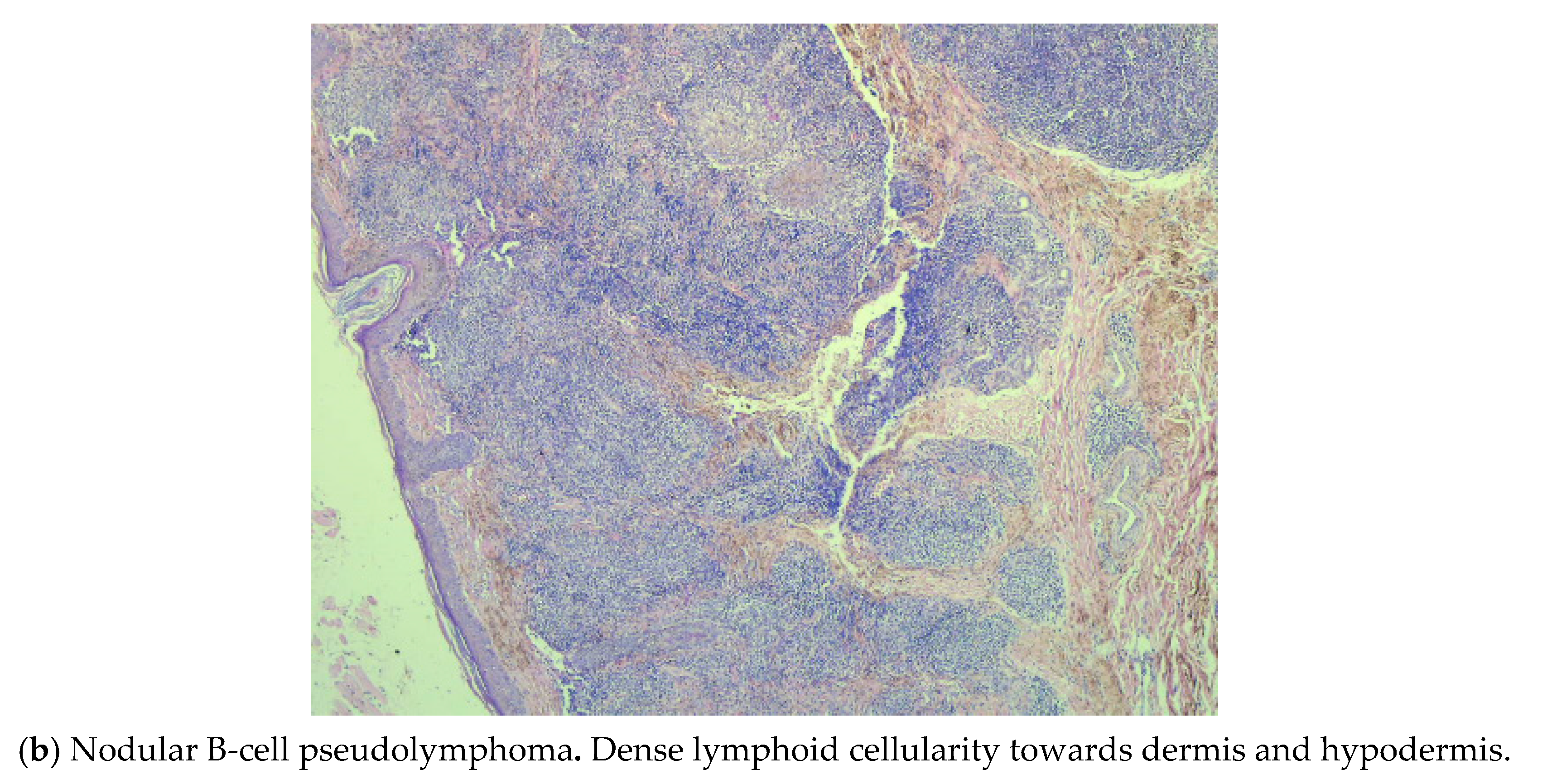
In the case of the suspected frontal sebaceous cyst, the immunohistochemistry test described a cutaneous pseudo lymphoma predominant with B lymphocytes associated with neoangiogenesis as shown in
Figure 1a,b.
From nine initially diagnosed BCC, two were described as ulcerated hemangiomas, two as squamous cell papillomas, four as actinic keratosis and one as a basal cell papilloma.
As mentioned before, one presumed SCC had a final histological diagnosis of pilomatrixoma. Pilomatrixoma, a benign tumor, known to occur in children, is rare in the middle-aged. Clinically and in aspiration cytology it is as a diagnostic pitfall. Correct preoperative diagnosis is 11–50% accurate and this often leads to unwarranted extensive surgery.
Pilomatrixoma, is a benign, calcifying, cutaneous tumor, originating from pluripotent precursors of the hair matrix cells of children and young adults. It has bimodal peak presentation, in the first and sixth decade, although can appear at any age [
6].
3.2. Basal Cell Carcinomas (BCC)
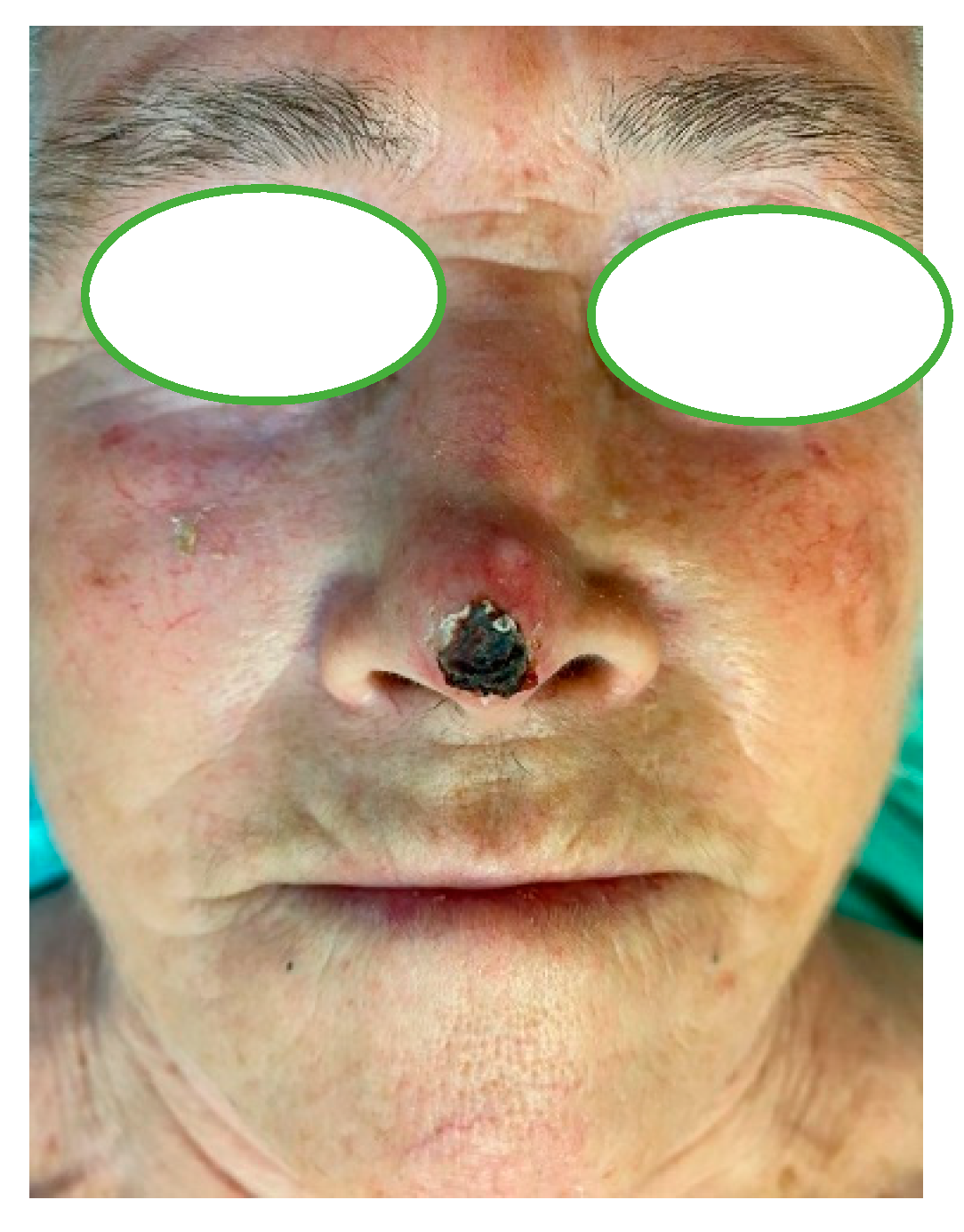
The facial localization of the BCC was variable. Therefore, 29 tumors were located in the orbito-palpebral region as follows: 18 corresponded with the internal angle of the orbit, seven with the upper and lower eyelid regions and two with the eyebrow region; 23 tumors had a nasogenian (14) or nasal (nasal wing—nine) localization; nine tumors were located in the zygomatic region, seven in the temporal region, one retroauricular and one on the ear pavilion as shown in
Figure 2 and
Figure 3.
Fifty-seven tumors were ulcerated and infected. Regarding the correspondence between the clinical diagnosis and the results of the anatomopathological exam, 62 tumors had the clinical diagnosis confirmed by the laboratory, seven tumors were presumed of being SCC but were later on identified as BCC and one suspicion of an ulcerated nasogenian melanoma was anatomopathologically described as a BCC.
The evolution of the basal cell carcinomas from the moment of debut to the time of initial diagnosis and excision varies as following: 48 cases had an evolution of over 10 years, 13 cases between 5–10 years and nine cases had an evolution of under 5 years.
3.3. Squamous Cell Carcinomas (SCC)
The clinical diagnoses corresponded with the pathological findings in 21 cases and differed in 15 cases, as follows: 12 tumors were presumed to be ulcerated BCC but were confirmed as SCC, one presumed preauricular SCC and one upper eyelid traumatized skin nevi were identified as malignant melanomas as shown in
Figure 4 and
Figure 5. Malignant melanoma is a widely spread skin tumor originating from the basal layer of melanocyte cells. It evolves in UV exposed skin and is often fatal. Rarely, the melanoma can also develop in other tissues, such as the lachrymal sac, uvea and mucous membranes, including the vulva, rectum, oral cavity, respiratory tract, and conjunctiva [
7]. Eyelid melanic tumors are pigmented skin nevi which, in certain situations (traumas, surgical interventions, inflammation) expand, become pruriginous and are surrounded by a vascularized halo and exulcerate; these being symptoms of malignancy [
8].
One presumed preauricular sarcoma was described by the laboratory as SCC.
The time of evolution from debut to surgical excision varied as follows: 21 cases had an evolution of over 2 years, nine cases between 1–2 years and five cases (including the melanoma) had an evolution of under 1 year.
To summarize, from the total of 226 tumors (both benign and malignant), 194 had the clinical diagnosis confirmed by the pathological exam and 34 had a different laboratory result from the clinical presumption: 10 benign tumors and 22 malignant tumors (eight BCC and 14 SCC, 12 of the latter being confused with ulcerovegetant BCC).
The National Comprehensive Cancer Network criteria for risk stratification includes different parameters, both clinical and pathologic, for separating BCC and CSCC into low- and high-risk lesions. Location, size and borders are the criteria that best correlated with pathology. For BCC and CSCC, cheek, forehead, scalp and neck lesions, under 10 mm, with well-defined borders were best correlated with low-risk lesions. BCC, over 10 mm in size, located on the forementioned areas, together with the central face, eyelids, eyebrows, nose, lips, temple, ears and with poorly defined borders, were associated with high-risk lesions.
The criteria for tumor clinical diagnosis included location of tumor, size, ulceration and changes in the neighboring skin. One of the most important factors was the evolution of the lesion over time.
4. Discussion
NMSC diagnosis is initially clinical, with histological confirmation following excision. The final diagnosis is always after the pathological examination, although the clinical aspect can suggest the tumor type. The ‘stretch test’ improves diagnostic accuracy in BCC. Dermatoscopy improves the accuracy of initial diagnostics in all NMSC and is helpful in determining the BCC sub-type. Pre-excisional tissue diagnosis can be indicative particularly for reconstruction if a graft or flap is required, or in an anatomically complex area such as the nose. This is best achieved by punch, incisional or shave biopsy under local anesthesia. Shave biopsy is to be avoided in possible cutaneous melanoma. Exfoliative cytology has a high diagnostic accuracy in NMSC when ulceration is present and guides the case management where surgical biopsy may be difficult, such as in the very elderly. A tissue sample diagnosis is required prior to radiotherapy (RT).
The nodular type of BCC is the most common form and may have clinical cystic or pigmented variants. Morphoeic BCCs are found almost exclusively on the head and neck, especially the nose. Superficial BCCs are found predominantly on the trunk. Basal cell carcinoma has a number of well-described histological subtypes.
The term ‘infiltrative BCC’ is used for all high-risk histological variants containing many BCCs of both high- and low-risk subtypes.
Cutaneous squamous cell carcinoma presents as a keratinizing indurated nodular or crusted tumor that may ulcerate, or it may present as an ulcer alone without evidence of keratinization. Nasal vestibule or ear canal localizations are often diagnosed late, with poor prognosis, as it can be misdiagnosed [
9].
After analyzing our data regarding the correspondence between the clinical and the histological diagnoses, we found that the majority of patients sought medical assistance very late; thus, establishing a high evolution time for aggressive malignant tumors (48 cases with over 10 years evolution for BCC and 21 cases with an evolution of over 2 years for CSCC). A higher evolution time leads to local tumor expansion along with ulcerated and infected tumors, therefore, making clinical evaluation difficult. Diagnosis of NMSC is usually clinical. Biopsy (exfoliative cytology) is recommended where the clinical diagnosis is uncertain, or where the histological features may influence the treatment and prior to radiation therapy (G) [
9]. Mohs surgery could be a good technique for skin tumors, especially for areas with high risk of recurrence such as the ear, temple, periauricular regions, retroauricular, nasolabial fold, nose, or upper lip. It is known to have the smallest recurrence rate of 3.4% to 7.9% and has the advantage of preserving healthy tissue, which is notably important, considering the aesthetic and functional outcomes; however, due to the technical issues we cannot apply it to our patients [
10].
Tumors that were clinically low risk, were correlated with pathological aspects of superficial, well defined growth patterns with no perineurial, lymphatic or vascular involvement. High risk tumors were poorly defined and associated with depth expansion as well as perineurial, lymphatic and vascular involvement.
Evaluating the aspects of clinical and pathological correlations and the predictive values of using clinical criteria for diagnosis, we found that using clinical means to detect a NMSC from a benign lesion had a positive predictive value (PPV) of 86%, and a negative predictive value of 76%. Clinically detecting BCC from other NMSCs had a PPV of 88%, and SCC from other NMSCs a PPV of 60%.
5. Conclusions
Despite extensive experience in the diagnosis and treatment of skin tumors, this is not always enough for matching the clinical and histological diagnoses. The high evolution time of malignant lesions, the ulcerated aspects of the tumors and the atypical localizations might lead to a lack of correspondence between the two diagnoses.
A pathological exam is mandatory after every skin lesion excision; as described above, and although benign tumors had a good correspondence (mismatches occurred mostly between different benign tumor types), between the clinical diagnosis of a benign lesion and the histological confirmation, there were several exceptions of histologically confirmed malignant lesions from lesions presumed benign.
The long-term goal of the study is to use our experience of correlating the clinical and the histological diagnosis in order to improve the existing knowledge on the differential diagnosis of both malignant and benign facial skin tumors.
Author Contributions
Conceptualization, C.T. and D.C.M.; methodology, A.T., V.I., C.L.I., B.M.C., I.M.J.H., I.T., C.S.; validation, C.T.; investigation, C.T., D.C.M., A.T., V.I., C.L.I., B.M.C., I.M.J.H., I.T., C.S., C.L.Z., C.T.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Ethics Commission of University of Medicine and Pharmacy “Grigore T. Popa” Iasi, 1 May 2018 in compliance with ethical and deontological rules for medical and research practice.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data published in this research are available on request from the first author and corresponding authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Apalla, Z.; Lallas, A.; Sotiriou, E.; Lazaridou, E.; Ioannides, D. Epidemiological trends in skin cancer. Dermatol. Pract. Concept. 2017, 7, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apalla, Z.; Nashan, D.; Weller, R.B.; Castellsagué, X. Skin Cancer: Epidemiology, Disease Burden, Pathophysiology, Diagnosis, and Therapeutic Approaches. Dermatol. Ther. 2017, 7 (Suppl. 1), 5–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sari, E. Non-metastatic Non-melanoma Skin Cancers: Our 3 Years of Clinical Experiences. World J. Plast. Surg. 2017, 6, 305–312. [Google Scholar] [PubMed]
- Matsuyama, Y.; Nakamura, T.; Hagi, T.; Asanuma, K.; Sudo, A. Subungual onychomycosis due to Aspergillus niger mimicking a glomus tumor: A case report. Biomed. Rep. 2017, 7, 532–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costea, C.F.; Petraru, D.; Dumitrescu, G.; Sava, A. Sebaceous carcinoma of the eyelid: Anatomoclinical data. Rom. J. Morphol. Embryol. 2013, 54, 665–668. [Google Scholar]
- Kumar, S. Rapidly growing pilomatrixoma on eyebrow. Indian J. Ophthalmol. 2008, 56, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Costea, C.F.; Anghel, K.; Dimitriu, G.; Dumitrescu, G.F.; Faiyad, Z.; Dumitrescu, A.; Sava, A. Anatomoclinical aspects of conjunctival malignant metastatic melanoma. Rom. J. Morphol. Embryol. 2014, 55, 933–937. [Google Scholar] [PubMed]
- Tiutiuca, C.; Voicu, D.; Brujbu, I.; Macovei, L.; Cupilan, C.; Bogdanici, C.; Bulimar, V. Malignant Tumors of the Eyeball and its Appendixes. Rev. Chim. (Buchar.) 2016, 67, 1641–1645. [Google Scholar]
- Newlands, C.; Currie, R.; Memon, A.; Whitaker, S.; Woolford, T. Non-melanoma skin cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130 (Suppl. 2), S125–S132. [Google Scholar] [CrossRef] [PubMed]
- Thorne, C.H.; Chung, K.C.; Gosain, A.K.; Gurtner, G.C. Grabb & Smith’s Plastic Surgery, 6th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; pp. 115–119. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 and
and 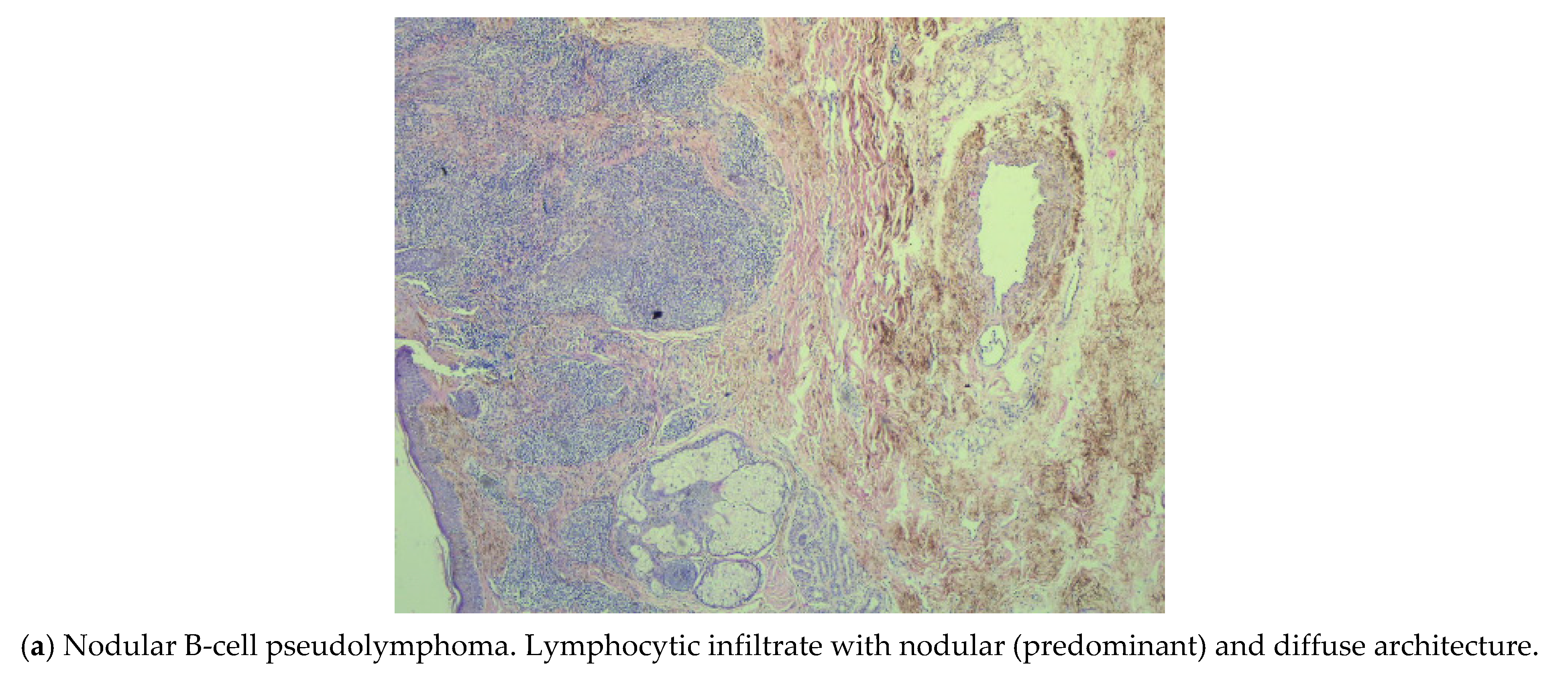{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





