
Struma Ovarii: Clinico-Morphological Features and Therapeutic Experience of a Romanian Institution over 20 Years

 ,
,
Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Discussion
4.1. Diagnosis Approach
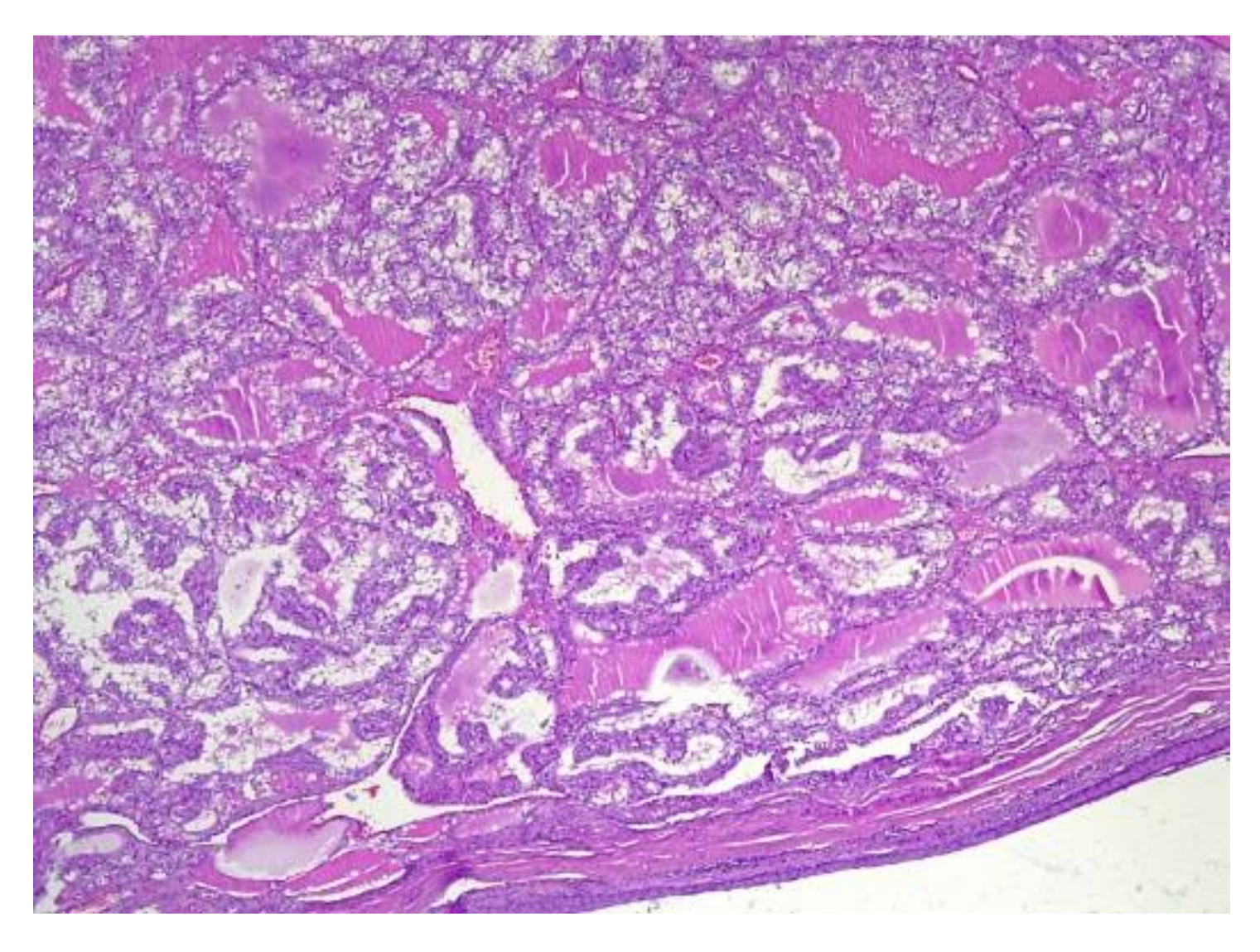
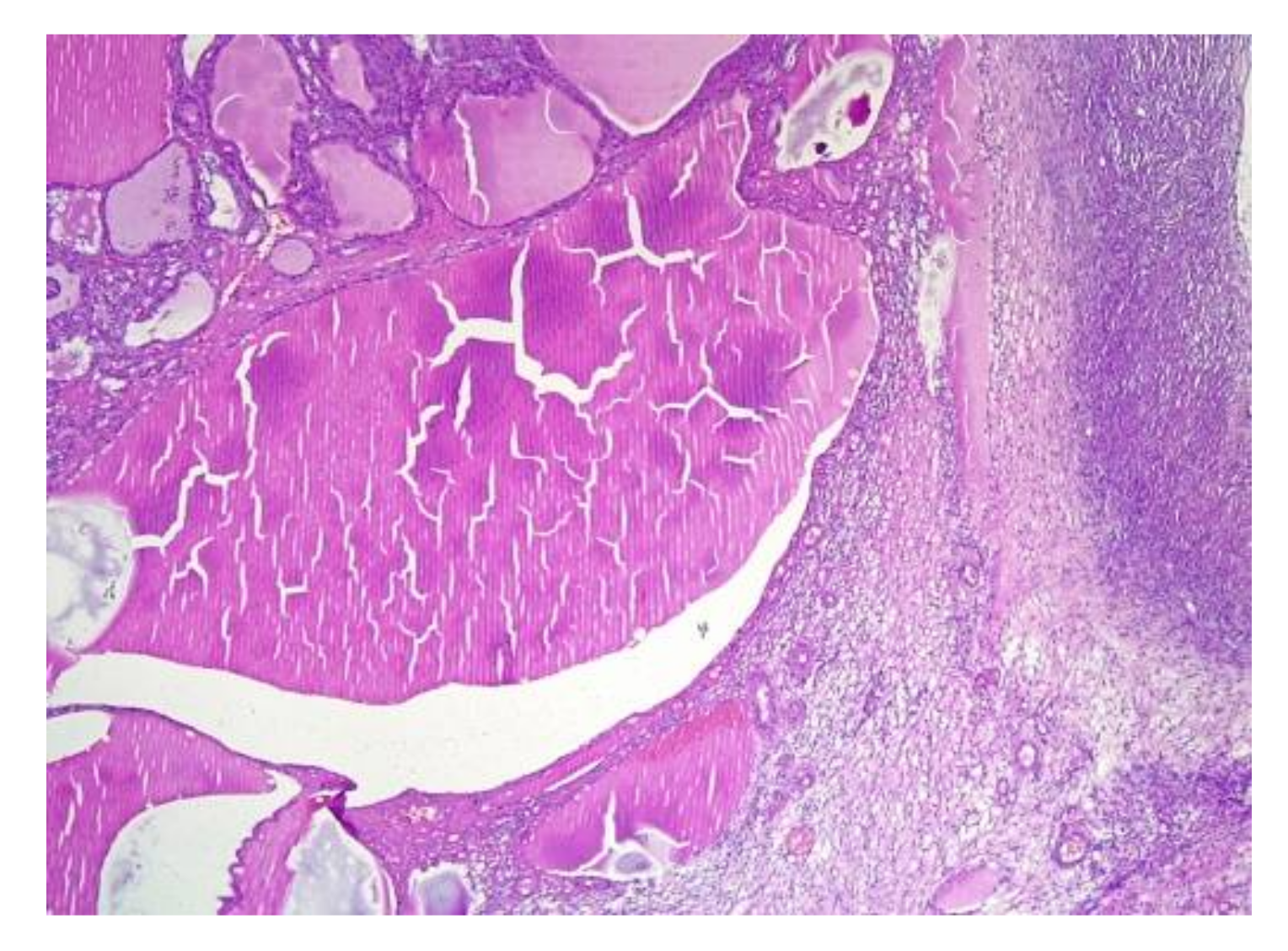
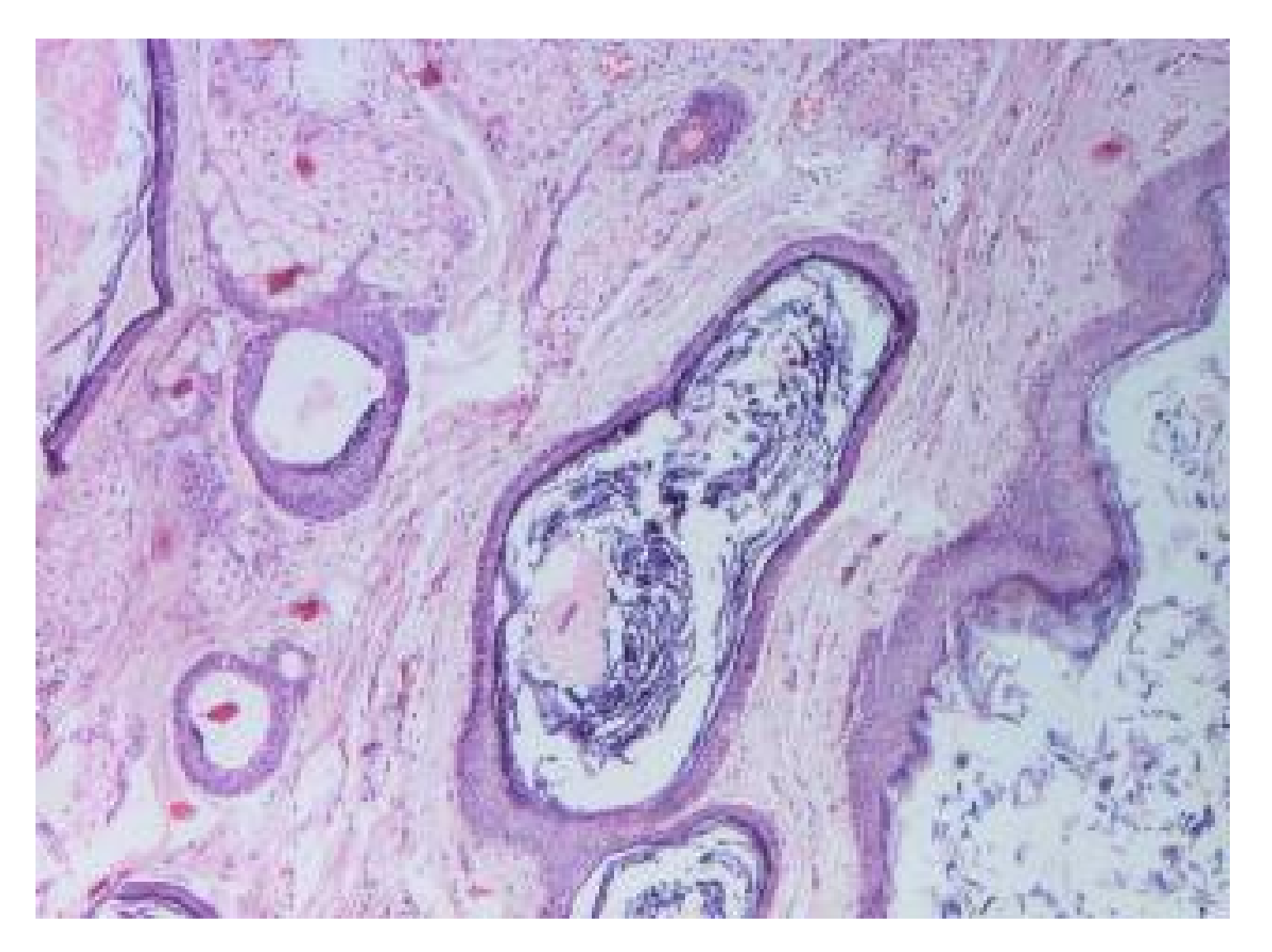
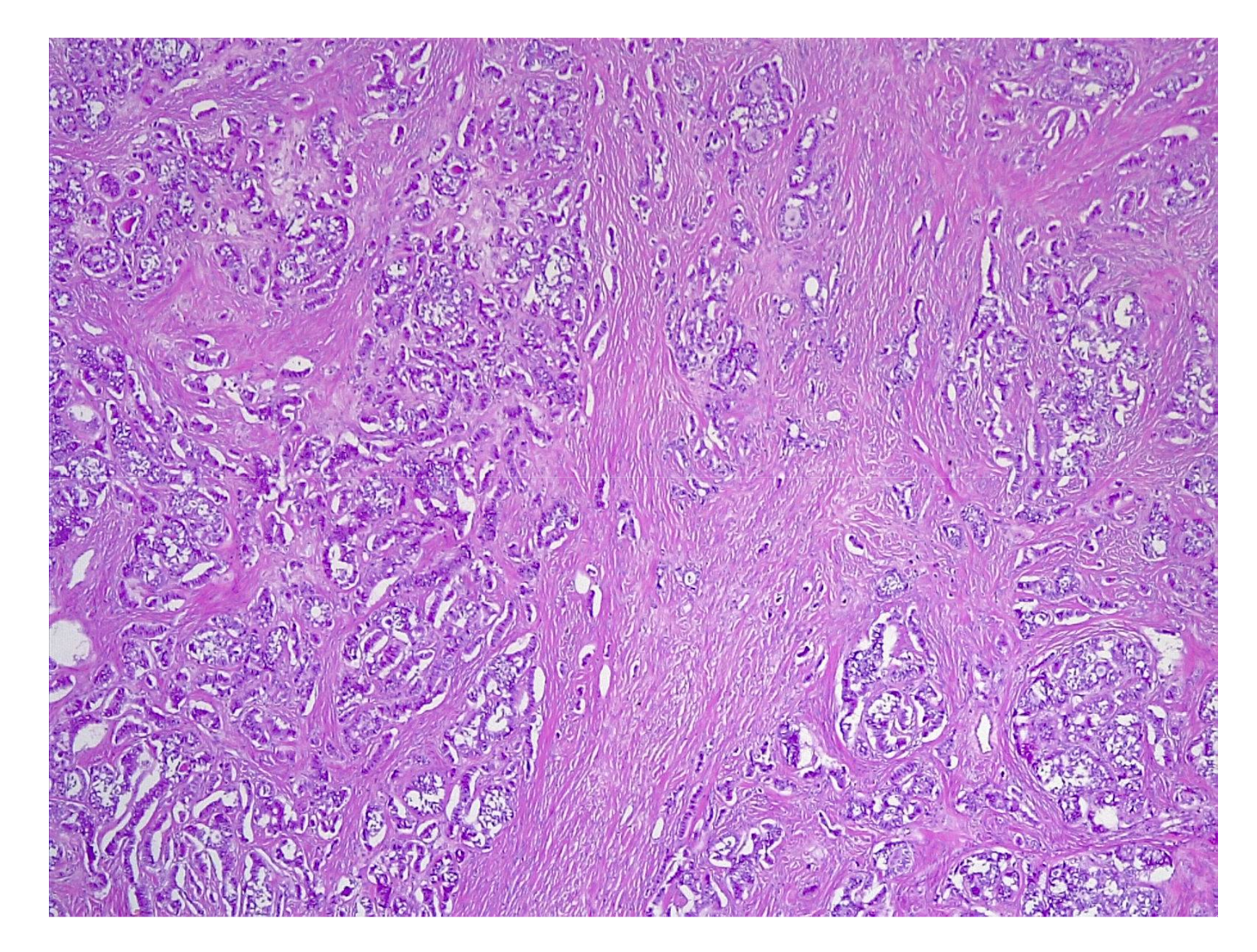
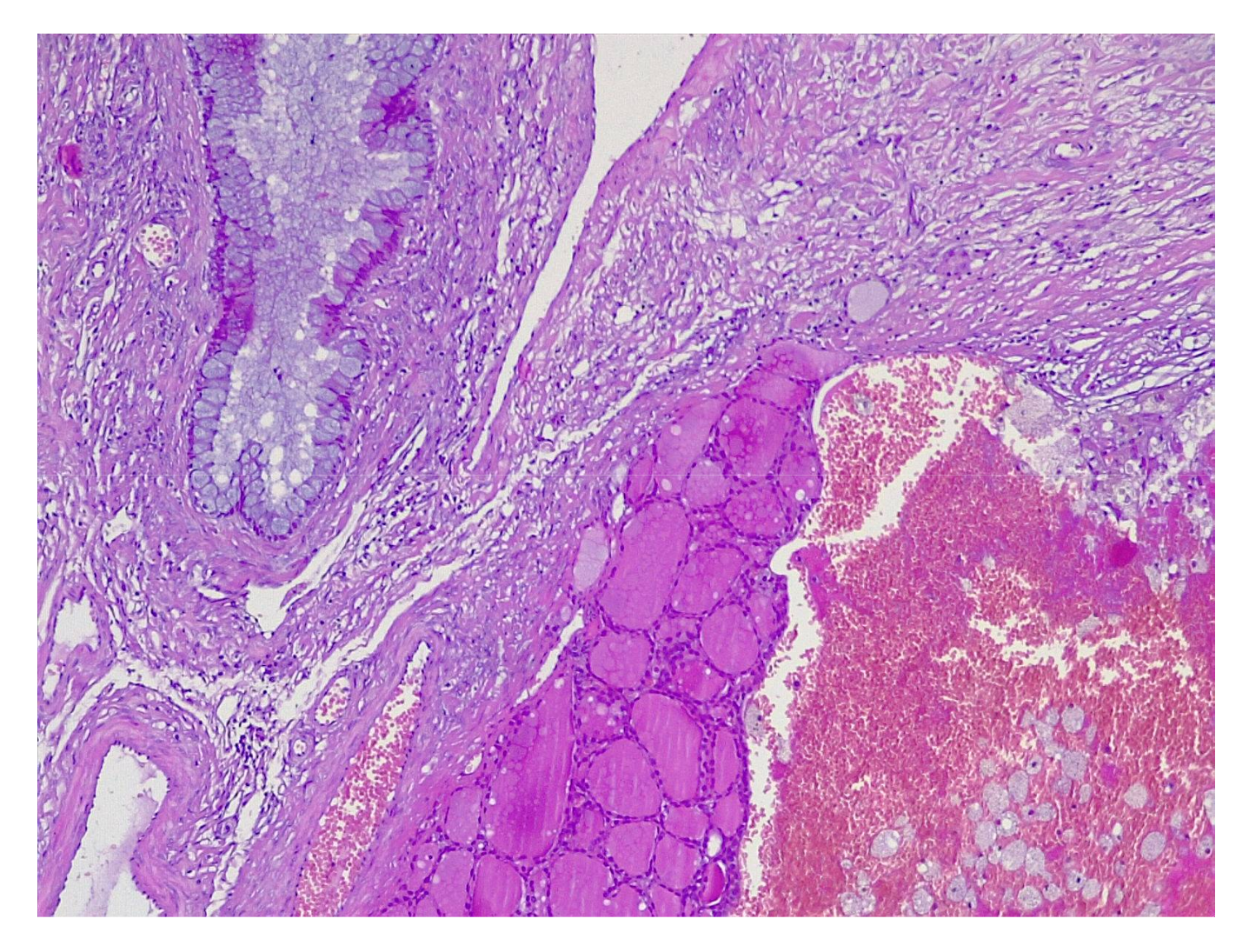
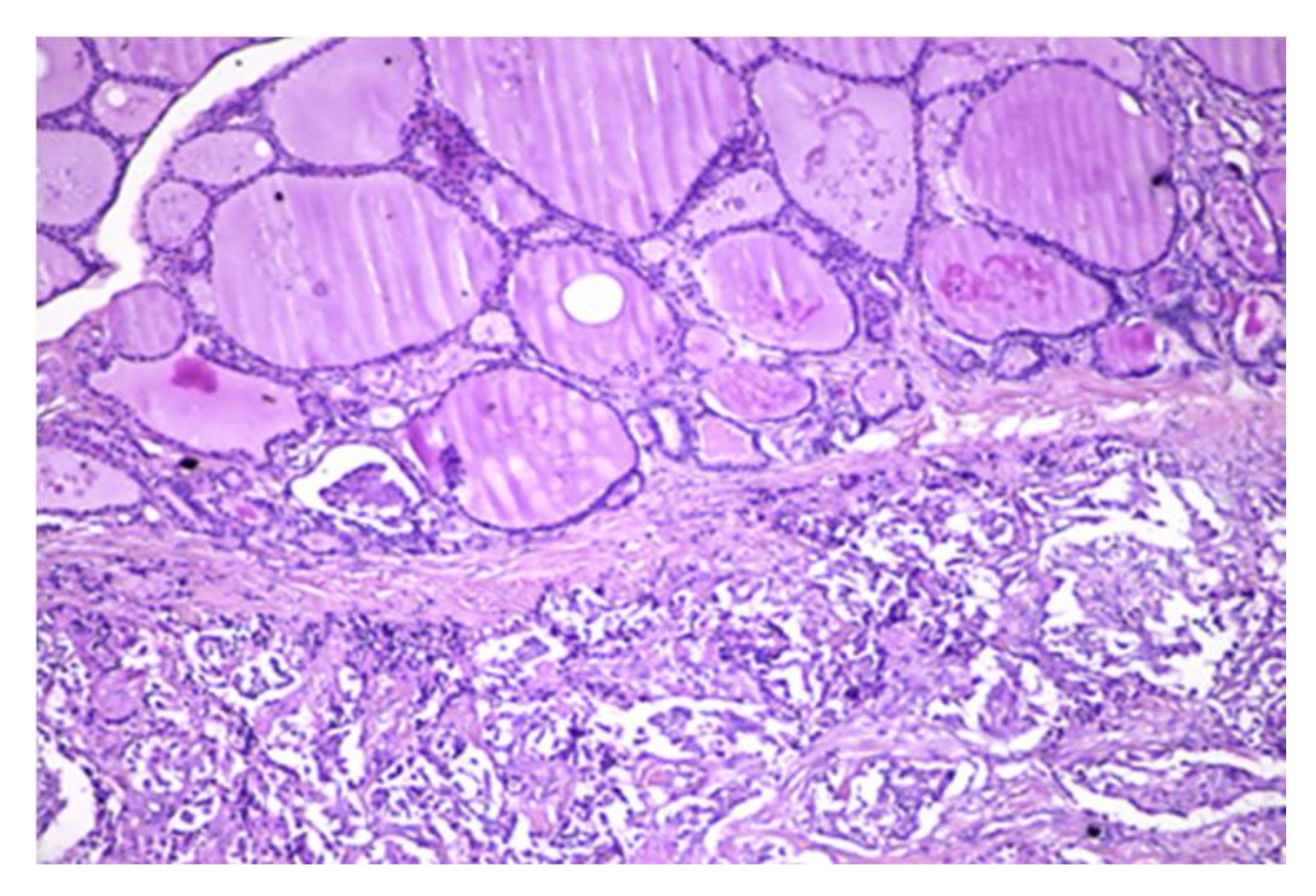
4.2. Histopathology Features
4.3. Treatment Strategies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamblin, G.; Gallice, C.; Bournaud, C.; Nadaud, B.; Lebail-Carval, K.; Chene, G. Benign struma ovarii: Report of 7 cases and review of the literature. Gynecol. Obstet. Fertil. 2016, 44, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Dujardin, M.I.; Sekhri, P.; Turnbull, L.W. Struma Ovarii: Role of imaging? Insights Imaging 2014, 5, 41–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, A.N.; Ellenson, L.H.; Gilks, C.B.; Kim, K.R.; Kong, C.S.; Lax, S.F.; Longacre, T.A.; Malpica, A.; McCluggage, W.G.; Oliva, E.; et al. Tumors of the Ovary. In Female Genital Tumours, 5th ed.; WHO Classification of Tumours Editorial Board, Ed.; International Agency for Research on Cancer: Lyon, France, 2020; Volume 4. [Google Scholar]
- Khatchapuridze, K.; Kekelidze, N.; Tsitsishvili, Z.; Mchedlishvili, M.; Kordzaia, D. Papillary Thyroid carcinoma in Struma Ovarii. Gynecol. Endocrinol. 2020, 36, 749–752. [Google Scholar] [CrossRef]
- Pastorino Casas, V.; Borghi Torzillo, M.F.; Schere, D.; Lutfi, R.J.; Faure, E.N. [Struma ovarii associated with Graves’ disease]. Medicina (B Aires) 2018, 78, 44–46. [Google Scholar]
- Deshpande, H.; Balkawade, N.; Gore, C.; Deshpande, A. Struma ovarii: A rare case report. Int. J. Pharm. Biomed. Sci. 2012, 3, 152–154. [Google Scholar]
- Boettlin, R. Uber zahnentwickelung in dermoid cysten des ovariums. Virchows Arch. Path. Arat. 1889, 115, 493–504. [Google Scholar] [CrossRef]
- Mandic, A.; Tesic, M.; Rajovic, J.; Vujkov, T.; Zivaljevic, M.; Mihajlevic, O.; Mutibaric, A. Ovarian teratomas: Struma ovarii. Arch. Oncol. 2001, 9, 189–191. [Google Scholar]
- Zaloudek, C. Tumors of ovary. In Diagnostic Histopathology of Tumors, 2nd ed.; Fletcher, C., Ed.; Churchill Livingstone: New York, NY, USA, 2000; p. 614. [Google Scholar]
- Wetteland, P. [Malignant struma ovarii]. Nord. Med. 1956, 56, 1568–1570. [Google Scholar]
- Niculescu, S.; Crauciuc, E.; Gargu, G.; Niculescu, D.; Filip, V.; Ene, D.; Vasilescu, A. [Struma ovarii]. Rev. Med. Chir. Soc. Med. Nat. Iasi 2008, 112, 406–410. [Google Scholar]
- Hosseini, A.; Moeini, A. Clinical finding and thyroid function in women with Struma ovarii. J. Cancer Res. 2013, 2013, 717584. [Google Scholar] [CrossRef] [Green Version]
- Zalel, Y.; Seidman, D.S.; Oren, M.; Achiron, R.; Gotlieb, W.; Mashiach, S.; Goldenberg, M. Sonographic and Clinical characteristics of Struma ovarii. J. Ultrasound Med. 2000, 19, 857–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, S.-C.; Chang, K.-H.; Lyu, M.-O.; Chang, S.-J.; Ryu, H.-S.; Kim, H.-S. Clinical characteristics of Struma ovarii. J. Gynecol. Oncol. 2008, 19, 135–138. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Pak, K.; Lim, H.J.; Yun, K.H.; Seong, S.J.; Kim, T.J.; Jung, H.W.; Park, I.S.; Shim, J.U.; Park, C.T.; et al. Clinical diversity of struma ovarii. Korean J. Obstet. Gynecol. 2002, 45, 748–752. [Google Scholar]
- Sinha, N.K. Struma ovarii with elevated Ca-125 levels and ascites mimicking advanced ca ovary. J. Clin. Diagn. Res. 2014, 8, 140–141. [Google Scholar] [CrossRef] [PubMed]
- Mimura, Y.; Kishida, M.; Masuyama, H.; Suwaki, N.; Kodama, J.; Otsuka, F.; Kataoka, H.; Yamauchi, T.; Ogura, T.; Kudo, T.; et al. Coexistence of Graves’ disease and Struma ovarii: Case report and literature review. Endocr. J. 2001, 48, 255–260. [Google Scholar] [CrossRef] [Green Version]
- Mui, M.P.; Tam, K.-F.; Tam, F.K.Y.; Ngan, H.Y.S. Coexistence of Struma ovarii with marked ascites and elevated CA-125 levels: Case report and literature review. Arch. Gynecol. Obstet. 2009, 279, 753–757. [Google Scholar] [CrossRef]
- Kougioumtsidou, A.; Kougioumtsidou, N.; Athanasopoulou, M.; Pados, G.; Tarlatzis, V. Struma ovarii in combination with increased levels of Ca125 and ascites: Case report and review of data of the literature. HJOG 2014, 13, 46–49. [Google Scholar]
- Saba, L.; Guerriero, S.; Sulcis, R.; Virgilio, B.; Melis, G.; Mallarini, G. Mature and immature ovarian teratomas: CT, US and MR imaging characteristics. Eur. J. Radiol. 2009, 72, 454–463. [Google Scholar] [CrossRef]
- Outwater, E.K.; Siegelman, E.S.; Hunt, J.L. Ovarian teratomas: Tumor types and imaging characteristics. Radiographics 2001, 21, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Xia, X.; Lin, Y.; Zhu, W.; Yuan, J. Diagnosis of Struma ovarii with medical imaging. Abdom. Imaging 2011, 36, 627–631. [Google Scholar] [CrossRef]
- Matsumoto, F.; Yoshioka, H.; Hamada, T.; Ishida, O.; Noda, K. Struma ovarii: CT and MR findings. J. Comput. Assist. Tomogr. 1990, 14, 310–312. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Kim, S.S.; Park, J.Y. MR Findings of Struma ovarii. Clin. Imaging. 2000, 24, 28–33. [Google Scholar] [CrossRef]
- Matsuki, M.; Kaji, Y.; Matsuo, M.; Kobashi, Y. Struma ovarii: MRI findings. Br. J. Radiol. 2000, 73, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Quddus, M.R.; Xiong, J.; Begun, S.M.K.N.; Lomme, M.; Hansen, K.; Sung, C.J.; Lawrence, W.D. Intra-operative consult for cystic struma ovarii-An experience in an academic medical center: A study of 53 cases over 21 years. OJOG 2013, 3, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Manini, C.; Magistris, A.; Puopolo, M.; Montironi, P.L. Cystic Struma ovarii: A report of three cases. Pathologica 2010, 102, 36–38. [Google Scholar]
- Roth, L.M.; Karseladze, A.I. Highly differentiated follicular carcinoma arising from Struma ovarii: A report of 3 cases, a review of the literature, and a reassessment of so-called peritoneal strumosis. Int. J. Gynecol. Pathol. 2008, 27, 213–222. [Google Scholar] [CrossRef]
- Roth, L.M.; Talerman, A. The enigma of struma ovarii. Pathology 2007, 39, 139–146. [Google Scholar] [CrossRef]
- Shaco-Levy, R.; Peng, R.Y.; Snyder, M.J.; Osmond, G.W.; Veras, E.; Bean, S.M.; Bentley, R.C.; Robboy, S.J. Malignant Struma ovarii: A blinded study of 86 cases assessing which histologic features correlate with aggressive clinical behavior. Arch. Pathol. Lab. Med. 2012, 136, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Mittra, E.S.; Niederkohr, R.D.; Rodriguez, C.; El-Maghraby, T.; McDougall, I.R. Uncommon causes of thyrotoxicosis. J. Nucl. Med. 2008, 49, 265–278. [Google Scholar] [CrossRef]
- Kraemer, B.; Grischke, E.-M.; Staebler, A.; Hirides, P.; Rothmund, R. Laparoscopic excision of malignant Struma ovarii and 1 year follow-up without further treatment. Fertil. Steril. 2011, 95, 2124.e9–2124.e12. [Google Scholar] [CrossRef]
- Nurliza, B.M.N.; Kusumoto, T.; Inoue, S.; Nakamura, K.; Seki, N.; Hongo, A.; Kodama, J.; Hiramatsu, Y. Three cases of struma ovarii underwent laparoscopic surgery with definite preoperative diagnosis. Acta Med. Okayama 2013, 67, 191–195. [Google Scholar] [CrossRef]
- Zhang, X.; Axiotis, C. Thyroid-type carcinoma of Struma ovarii. Arch. Pathol. Lab. Med. 2010, 134, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Zarkavelis, G.; Seraj, E.; Zerdes, I.; Tatsi, K.; Pentheroudakis, G. Non-epithelial ovarian cancer: Elucidating uncommon gynaecological malignancies. Anticancer Res. 2016, 36, 5031–5042. [Google Scholar] [CrossRef] [Green Version]
- McGill, J.F.; Sturgeon, C.; Angelos, P. Metastatic Struma ovarii Treated with total thyroidectomy and radioiodine ablation. Endocr. Pract. 2009, 15, 167–173. [Google Scholar] [CrossRef]
- Merza, Z.; White, D.; Khanem, N. Struma ovarii in pregnancy: An uncommon cause of hyperthyroidism. Clin. Nucl. Med. 2015, 40, 687–688. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Moschetta, M.; Tatsi, K.; Tsiouris, A.K.; Pavlidis, N. A Review on pregnancy complicated by ovarian epithelial and non-epithelial malignant tumors: Diagnostic and therapeutic perspectives. J. Adv. Res. 2018, 12, 1–9. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Nr | Age of Patients (Years) | Ovary | The Largest Tumor Size (cm) | Year of Diagnosis | Additional Conditions to Struma Ovarii | CA-125 (Ui/mL) |
|---|---|---|---|---|---|---|
| 1 | 43 | left | 18 | 2001 | Serous cystadenoma | 4.94 |
| 2 | 28 | right | 4.5 | 2001 | Uterin leiomiomatosis | |
| 3 | 41 | right | 8 | 2003 | Mucinous cystadenoma | 10.7 |
| 4 | 71 | right | 6 | 2004 | Mucinous cystadenoma | 14.6 |
| 5 | 49 | left | 8 | 2004 | - | 3.7 |
| 6 | 51 | right | 10 | 2005 | Serous cystadenoma Ascites | 45 |
| 7 | 35 | left | 2.5 | 2005 | Ovarian torsion Hyperthyroidism | 5.2 |
| 8 | 42 | left | 1 | 2005 | - | 3.1 |
| 9 | 26 | left | 7 | 2006 | Ovarian torsion | 4.2 |
| 10 | 32 | left | 5 | 2006 | Thyroid papillary carcinoma | 22.6 |
| 11 | 45 | left | 3.5 | 2007 | Uterin leiomiomatosis | 9.4 |
| 12 | 33 | right | 9 | 2007 | Cystic teratoma Chronic inflammation | 15.9 |
| 13 | 68 | left | 9 | 2007 | Surface papilomatosis Peritoneal implants | 18.4 |
| 14 | 42 | left | 4 | 2008 | Teratoma | 8.9 |
| 15 | 38 | left | 7 | 2009 | Teratoma Serous cystadenoma | 9.2 |
| 16 | 27 | right | 6 | 2010 | Pregnancy Serouse cystadenoma | 5.6 |
| 17 | 50 | left | 20 | 2010 | - | 3.6 |
| 18 | 46 | left | 5 | 2011 | Serous cystadenoma | 11.2 |
| 19 | 33 | right | 10 | 2015 | Pregnancy | 10.8 |
| 20 | 24 | right | 8 | 2016 | Mucinous cystadenoma Strumal carcinoid | 38 |
| 21 | 42 | right | 3,5 | 2018 | Teratoma | 8.2 |
| 22 | 54 | right + left | 18 | 2019 | - | 4.1 |
| 23 | 31 | right | 9 | 2019 | Pregnancy Ovarian torsion | 6.4 |
| 24 | 54 | left | 11 | 2019 | Teratoma Hyperthyroidism | 11.5 |
| 25 | 59 | right | 3.7 | 2021 | Strumal carcinoid | 19.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tîrnovanu, M.C.; Tîrnovanu, V.G.; Toma, B.F.; Cojocaru, E.; Ungureanu, C.; Barbăroșie, C.; Lozneanu, L. Struma Ovarii: Clinico-Morphological Features and Therapeutic Experience of a Romanian Institution over 20 Years. Appl. Sci. 2021, 11, 9427. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209427
Tîrnovanu MC, Tîrnovanu VG, Toma BF, Cojocaru E, Ungureanu C, Barbăroșie C, Lozneanu L. Struma Ovarii: Clinico-Morphological Features and Therapeutic Experience of a Romanian Institution over 20 Years. Applied Sciences. 2021; 11(20):9427. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209427
Chicago/Turabian StyleTîrnovanu, Mihaela Camelia, Vlad Gabriel Tîrnovanu, Bogdan Florin Toma, Elena Cojocaru, Carmen Ungureanu, Cătălina Barbăroșie, and Ludmila Lozneanu. 2021. "Struma Ovarii: Clinico-Morphological Features and Therapeutic Experience of a Romanian Institution over 20 Years" Applied Sciences 11, no. 20: 9427. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209427