
Choroidal Vascularity Index in Adult-Onset Foveomacular Vitelliform Dystrophy: A Pilot Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
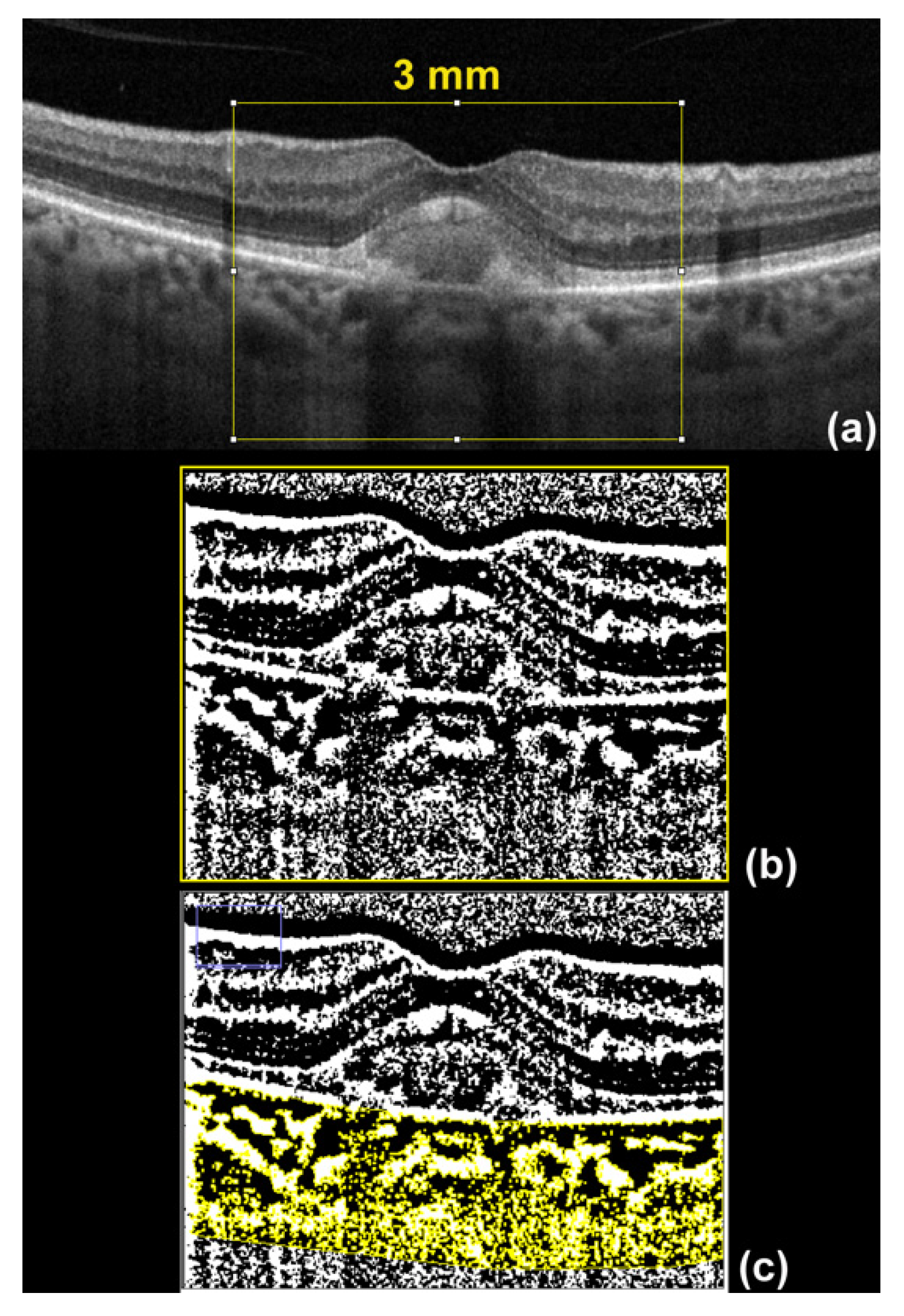
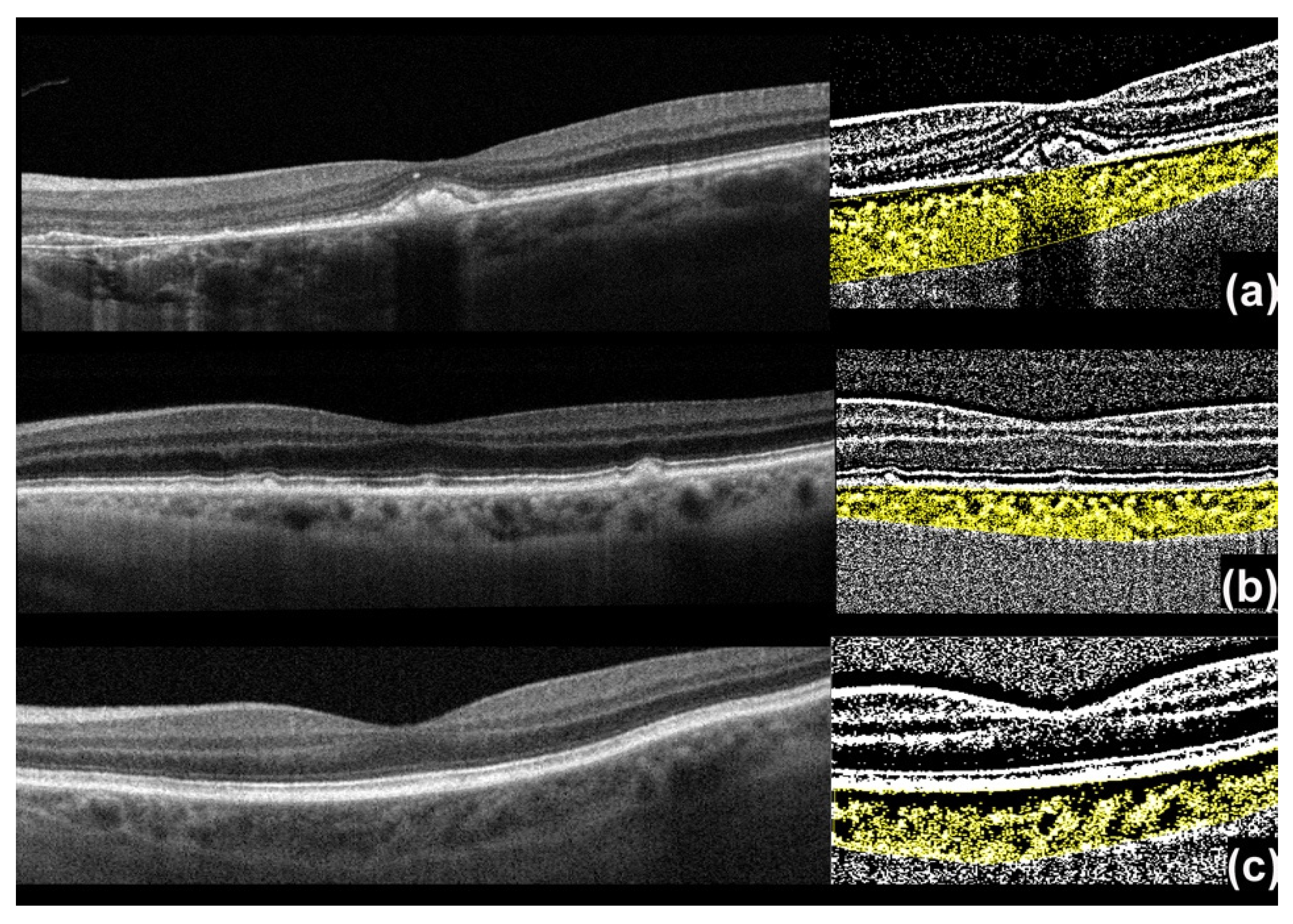
2.1. Imaging Processing
2.2. Choroidal Vascularity Index (CVI) Assessment
2.3. Statistical Analysis
3. Results
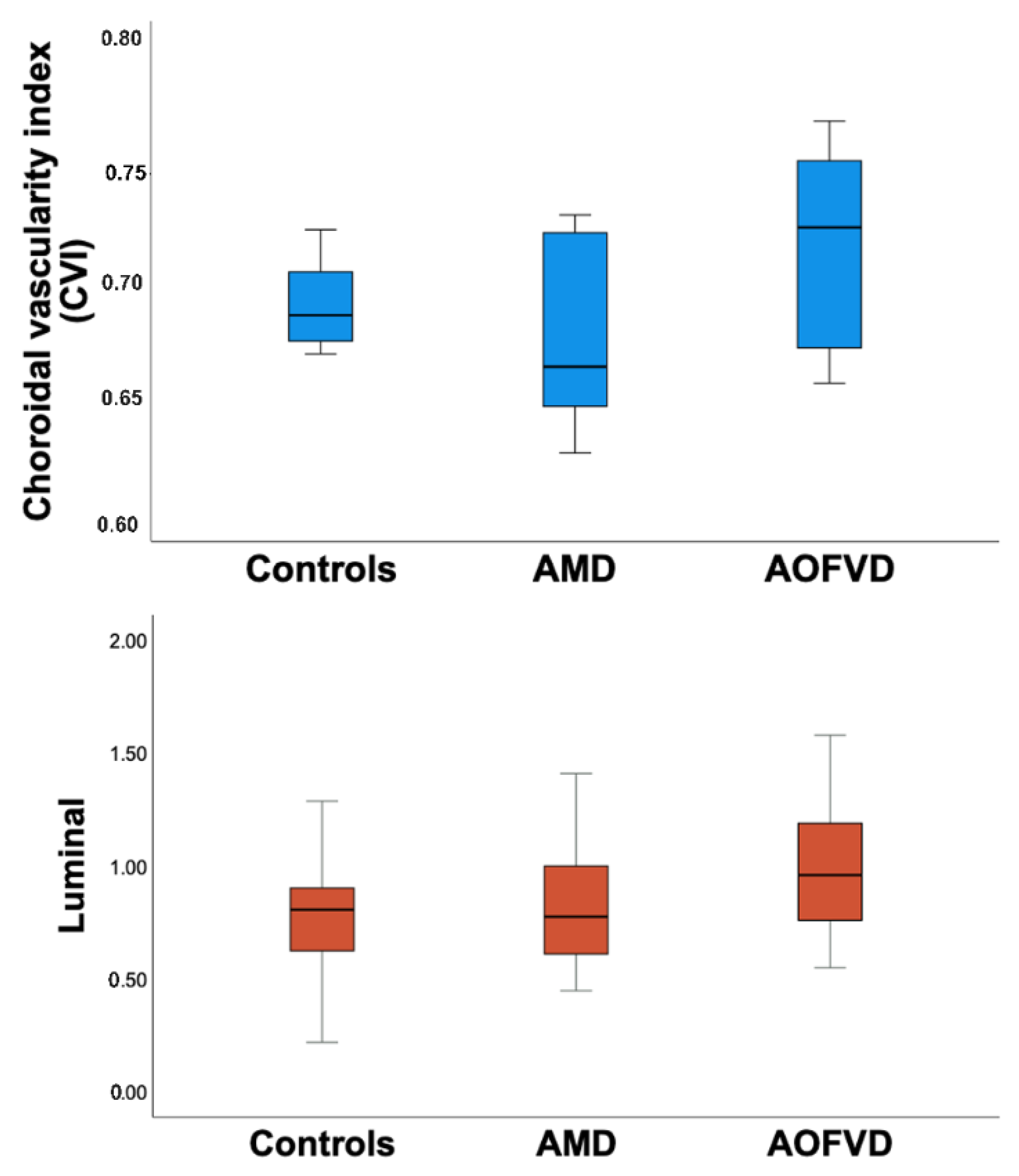
Analysis of Choroidal Vasculature
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gass, J.D. A clinicopathologic study of a peculiar foveomacular dystrophy. Trans. Am. Ophthalmol. Soc. 1974, 72, 139–156. [Google Scholar] [PubMed]
- Chowers, I.; Tiosano, L.; Audo, I.; Grunin, M.; Boon, C. Adult-onset foveomacular vitelliform dystrophy: A fresh perspective. Prog. Retin. Eye Res. 2015, 47, 64–85. [Google Scholar] [CrossRef] [PubMed]
- Querques, G.; Forte, R.; Querques, L.; Massamba, N.; Souied, E.H. Natural Course of Adult-Onset Foveomacular Vitelliform Dystrophy: A Spectral-Domain Optical Coherence Tomography Analysis. Am. J. Ophthalmol. 2011, 152, 304–313. [Google Scholar] [CrossRef]
- Ozcaliskan, S.; Balci, S.; Yenerel, N.M. Choroidal vascularity index determined by binarization of enhanced depth imaging optical coherence tomography images in eyes with intermediate age-related macular degeneration. Eur. J. Ophthalmol. 2020, 30, 1512–1518. [Google Scholar] [CrossRef]
- Querques, G.; Querques, L.; Forte, R.; Massamba, N.; Coscas, F.; Souied, E.H. Choroidal Changes Associated with Reticular Pseudodrusen. Investig. Opthalmol. Vis. Sci. 2012, 53, 1258–1263. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, R.; Chhablani, J.; Chintan, S.; Shah, S.; Sarvaiya, C.; Banker, A. CHOROIDAL VASCULARITY INDEX IN CENTRAL SEROUS CHORIORETINOPATHY. Retina 2016, 36, 1646–1651. [Google Scholar] [CrossRef]
- Coscas, F.; Puche, N.; Coscas, G.; Srour, M.; Français, C.; Glacet-Bernard, A.; Querques, G.; Souied, E.H. Comparison of Macular Choroidal Thickness in Adult Onset Foveomacular Vitelliform Dystrophy and Age-Related Macular Degeneration. Investig. Opthalmol. Vis. Sci. 2014, 55, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grenga, P.L.; Fragiotta, S.; Cutini, A.; Meduri, A.; Vingolo, E.M. Enhanced Depth Imaging Optical Coherence Tomography in Adult-Onset Foveomacular Vitelliform Dystrophy. Eur. J. Ophthalmol. 2015, 26, 145–151. [Google Scholar] [CrossRef]
- Palácios, R.M.; Mendes, T.S.; Sano, R.Y.; Wu, D.C.; Aihara, T.; Manzano, R.P.D.A. Choroidal thickness using EDI-OCT in adult-onset vitelliform macular dystrophy. Int. J. Retin. Vitr. 2016, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Cennamo, G.; Montorio, D.; Mirra, F.; Comune, C.; D’Alessandro, A.; Tranfa, F. Study of vessel density in adult-onset foveomacular vitelliform dystrophy with optical coherence tomography angiography. Photodiagnosis Photodyn. Ther. 2020, 30, 101702. [Google Scholar] [CrossRef]
- Sonoda, S.; Sakamoto, T.; Yamashita, T.; Uchino, E.; Kawano, H.; Yoshihara, N.; Terasaki, H.; Shirasawa, M.; Tomita, M.; Ishibashi, T. Luminal and Stromal Areas of Choroid Determined by Binarization Method of Optical Coherence Tomographic Images. Am. J. Ophthalmol. 2015, 159, 1123–1131.e1. [Google Scholar] [CrossRef]
- Branchini, L.A.; Adhi, M.; Regatieri, C.; Nandakumar, N.; Liu, J.J.; Laver, N.; Fujimoto, J.G.; Duker, J.S. Analysis of Choroidal Morphologic Features and Vasculature in Healthy Eyes Using Spectral-Domain Optical Coherence Tomography. Ophthalmology 2013, 120, 1901–1908. [Google Scholar] [CrossRef]
- Iovino, C.; Pellegrini, M.; Bernabei, F.; Borrelli, E.; Sacconi, R.; Govetto, A.; Vagge, A.; Di Zazzo, A.; Forlini, M.; Finocchio, L.; et al. Choroidal Vascularity Index: An In-Depth Analysis of This Novel Optical Coherence Tomography Parameter. J. Clin. Med. 2020, 9, 595. [Google Scholar] [CrossRef] [Green Version]
- Sonoda, S.; Sakamoto, T.; Yamashita, T.; Shirasawa, M.; Uchino, E.; Terasaki, H.; Tomita, M. Choroidal Structure in Normal Eyes and After Photodynamic Therapy Determined by Binarization of Optical Coherence Tomographic Images. Investig. Opthalmol. Vis. Sci. 2014, 55, 3893–3899. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Wei, X.; Goud, A.; Vupparaboina, K.K.; Jana, S.; Chhablani, J. Influence of scanning area on choroidal vascularity index measurement using optical coherence tomography. Acta Ophthalmol. 2017, 95, e770–e775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, X.; Sonoda, S.; Mishra, C.; Khandelwal, N.; Kim, R.; Sakamoto, T.; Agrawal, R. Comparison of Choroidal Vascularity Markers on Optical Coherence Tomography Using Two-Image Binarization Techniques. Investig. Opthalmol. Vis. Sci. 2018, 59, 1206–1211. [Google Scholar] [CrossRef] [Green Version]
- Puche, N.; Querques, G.; Blanco-Garavito, R.; Zerbib, J.; Gherdaoui, F.; Tilleul, J.; Coscas, F.; Glacet-Bernard, A.; Souied, E.H. En face enhanced depth imaging optical coherence tomography features in adult onset foveomacular vitelliform dystrophy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 252, 555–562. [Google Scholar] [CrossRef]
- Parodi, M.B.; Rabiolo, A.; Cicinelli, M.V.; Iacono, P.; Romano, F.; Bandello, F. Quantitative analysis of optical coherence tomography angiography in adult-onset foveomacular vitelliform dystrophy. Retina 2018, 38, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Querques, G.; Zambrowski, O.; Corvi, F.; Miere, A.; Semoun, O.; Srour, M.; Souied, E.H. Optical coherence tomography angiography in adult-onset foveomacular vitelliform dystrophy. Br. J. Ophthalmol. 2016, 100, 1724–1730. [Google Scholar] [CrossRef]
- Carnevali, A.; Al-Dolat, W.; Sacconi, R.; Corbelli, E.; Querques, L.; Bandello, F.; Querques, G. Diagnosis, management and future treatment options for adult-onset foveomacular vitelliform dystrophy. Expert Rev. Ophthalmol. 2018, 13, 161–169. [Google Scholar] [CrossRef]
- Rabiolo, A.; Carnevali, A.; Bandello, F.; Querques, G. Optical Coherence Tomography Angiography: Evolution or Revolution? Expert Rev. Ophthalmol. 2016, 11, 243–245. [Google Scholar] [CrossRef] [Green Version]
- Carnevali, A.; Mastropasqua, R.; Gatti, V.; Vaccaro, S.; Mancini, A.; D’Aloisio, R.; Lupidi, M.; Cerquaglia, A.; Sacconi, R.; Borrelli, E.; et al. Optical Coherence Tomography Angiography in Intermediate and Late Age-Related Macular Degeneration: Review of Current Technical Aspects and Applications. Appl. Sci. 2020, 10, 8865. [Google Scholar] [CrossRef]
- Nickla, D.L.; Wildsoet, C.F.; Troilo, D. Diurnal rhythms in intraocular pressure, axial length, and choroidal thickness in a primate model of eye growth, the common marmoset. Investig. Ophthalmol. Vis. Sci. 2002, 43, 2519–2528. [Google Scholar]
- Altinkaynak, H.; Ceylan, E.; Kartal, B.; Keles, S.; Ekinci, M.; Olcaysü, O.O.; Altınkaynak, H. Measurement of Choroidal Thickness Following Caffeine Intake in Healthy Subjects. Curr. Eye Res. 2015, 41, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nagasato, D.; Mitamura, Y.; Egawa, M.; Kameoka, M.; Nagasawa, T.; Tabuchi, H.; Kinoshita, T.; Sonoda, S.; Sakamoto, T. Changes of choroidal structure and circulation after water drinking test in normal eyes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 2391–2399. [Google Scholar] [CrossRef]
- Dubovy, S.R.; Hairston, R.J.; Schatz, H.; Schachat, A.P.; Bressler, N.M.; Finkelstein, D.; Green, W.R. Adult-onset foveomacular pigment epithelial dystrophy. Retina 2000, 20, 638–649. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.J.; Sarks, J.P.; Killingsworth, M.C.; Kettle, E.K.; Sarks, S.H. Adult vitelliform macular degeneration: A clinicopathological study. Eye 2003, 17, 717–726. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | AOFVD | AMD | Controls | p Value |
|---|---|---|---|---|
| No. of eyes | 18 | 18 | 16 | |
| No. of patients | 18 | 18 | 16 | |
| Age (years) | 74.6 ± 9.2 | 76.1 ± 13 | 76.4 ± 6.9 | 0.80 |
| Gender (female) | 10 (55.5%) | 9 (50%) | 9 (56.2%) | 0.06 |
| Feature | AOFVD N = 18 | AMD N = 18 | Controls N = 16 | p Value |
|---|---|---|---|---|
| Luminal Area | 1.05 ± 0.39 | 0.83 ± 0.27 | 0.77 ± 0.26 | 0.04 |
| Total area | 1.46 ± 0.48 | 1.25 ± 0.43 | 1.12 ± 0.36 | 0.07 |
| CVI | 0.71 ± 0.04 | 0.68 ± 0.03 | 0.69 ± 0.02 | 0.004 |
| SFCT | 215.4 ± 52.2 | 196.9 ± 64.3 | 230.5 ± 68.4 | 0.29 |
| CT N 500 | 226.5 ± 61.3 | 180. 5 ± 66.7 | 213.6 ± 61.9 | 0.09 |
| CT T 500 | 221.8 ± 53.3 | 202.4 ± 56.4 | 207.1 ± 60.3 | 0.57 |
| CT N 1500 | 210.1 ± 68.9 | 155.7 ± 70.9 | 213.5 ± 74.6 | 0.04 |
| CT T 1500 | 206.1 ± 57.2 | 206.7 ± 50.1 | 191.3 ± 73.8 | 0.71 |
| Feature | AOFVD N = 18 | AMD N = 18 | ||
|---|---|---|---|---|
| p value | p value | |||
| Luminal Area | AMD | 0.05 | AOFVD: | 0.05 |
| Control | 0.02 | Control: | 0.63 | |
| CVI | AMD | 0.001 | AOFVD: | 0.001 |
| Control | 0.03 | Control: | 0.25 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdolrahimzadeh, S.; Fragiotta, S.; Ciacimino, C.; Di Pippo, M.; Scuderi, G. Choroidal Vascularity Index in Adult-Onset Foveomacular Vitelliform Dystrophy: A Pilot Study. Appl. Sci. 2021, 11, 10487. https://0-doi-org.brum.beds.ac.uk/10.3390/app112110487
Abdolrahimzadeh S, Fragiotta S, Ciacimino C, Di Pippo M, Scuderi G. Choroidal Vascularity Index in Adult-Onset Foveomacular Vitelliform Dystrophy: A Pilot Study. Applied Sciences. 2021; 11(21):10487. https://0-doi-org.brum.beds.ac.uk/10.3390/app112110487
Chicago/Turabian StyleAbdolrahimzadeh, Solmaz, Serena Fragiotta, Chiara Ciacimino, Mariachiara Di Pippo, and Gianluca Scuderi. 2021. "Choroidal Vascularity Index in Adult-Onset Foveomacular Vitelliform Dystrophy: A Pilot Study" Applied Sciences 11, no. 21: 10487. https://0-doi-org.brum.beds.ac.uk/10.3390/app112110487