
The Wearable Physical Fitness Training Device Based on Fuzzy Theory


1
Department of Computer Science & Information Engineering, National Quemoy University, Kinmen 892009, Taiwan
2
Department of Electrical Engineering, National Taiwan Ocean University, Keelung 202301, Taiwan
3
Center of Excellence for Ocean Engineering, National Taiwan Ocean University, Keelung 202301, Taiwan
4
Computer Science and Engineering, National Taiwan Ocean University, Keelung 202301, Taiwan
5
Department of Computer Science and Information Engineering, National Taipei University of Technology, Taipei 106331, Taiwan
*
Authors to whom correspondence should be addressed.
Appl. Sci. 2021, 11(21), 9976; https://0-doi-org.brum.beds.ac.uk/10.3390/app11219976
Submission received: 21 July 2021
/
Revised: 15 October 2021
/
Accepted: 15 October 2021
/
Published: 25 October 2021
(This article belongs to the Special Issue Intelligent Systems and Applications of Data Science and Internet of Things Techniques Ⅱ)
Abstract
:Mobile Edge Computing and Communication (MECC) can be deployed in close proximity with sensing devices and act as middleware between cloud and local networks. The health and fitness movement has become extremely popular recently. Endurance activities, such as marathons, triathlons, and cycling have also grown in popularity. However, with more people participating in these activities, more accidents and injuries occur—ranging from heat stroke, to heart attacks, shock, or hypoxia. All physical training activities include a risk of injury and accidents. Therefore, any research that offers a means of reducing injury risk will significantly contribute to the personal fitness field. Moreover, with the growing popularity of wearable devices and the rise of the MECC, the development and application of wearable devices that can connect to the MECC has become widespread, producing many new innovations. Although many wearable devices, such as wrist straps and smart watches, are available and able to detect individual physiological data, they cannot monitor the human body in a state of motion. Therefore, this study proposes a set of monitoring parameters for a novel wearable device connected to the MECC based on fitness management to assist fitness trainers in effective prompted strength training, and to offer timely warnings in the event of an injury risk. The data collected by the monitoring device using fuzzy theory include risk factor, body temperature, heart rate, and blood oxygen concentration. The proposed system can display in real-time the current physiological state of a wearer/user. The introduction of this device will hopefully enable trainers to immediately and effectively control and monitor the intensity of a training session, while increasing training safety, and offer crucial and immediate diagnostic information so that the correct treatment can be applied without delay in the event of injury.
1. Introduction
In recent years, sport activities have become popular among the general public, and intense training in sports is no longer exclusively undertaken by professional sportspersons. Although professionals have the benefit of having the best coaching staff, others do not, resulting in sports injuries and accidents caused by excessive exercise and improper training [1]. Ref. [1] suggested that the same parameters of exercise (intensity, duration, and frequency) that determine the positive fitness and health effects of physical training also appear to influence the risk of injuries. In addition, some studies of runners and other physically active groups have consistently demonstrated that greater duration and frequency of exercise are associated with higher risks of injury. Given that each body or the degree of feeling in an environment vary, training can be quantified using units, such as mathematics and monitoring [2], mastering training methods, intensity, and so on. The main motivation of this research is the proposal of a novel monitoring system that allows a trainer to make appropriate adjustments to these measures to avoid training injuries.
The human body is a complex biological system where each organ has interrelated activities. A person undertaking training experiences a unique combination of internal–external factors according to the intensity of that training [3]. Trainers may have “a feel” for determining workout intensity, which is the product of training and experience. However, this feeling can never provide a sufficiently accurate understanding of how a trainee’s body is reacting to the workout intensity to predict and prevent injury [4]. Injury risk in sports is not affected by a single factor, but is the product of a combination of factors, such as body temperature, heartbeat, blood oxygen level, changes in temperature, and humidity in the environment. All of these factors [4] may combine in such a way as to cause dangerous physiological changes in the human body, resulting in injury. We have the following statements.
- Each sensor can only make state judgments based on the range of sensing values, and it is not possible to know the physical state of the subject only by a single sensor. In this paper, the measured value of each sensor is converted into a state, and the Fuzzy theory is used to comprehensively evaluate the physical fitness. A single state of badness may not cause the body harm, but many states of badness may cause the body harm, and real-time physical fitness can provide subject with a way to predict and prevent injuries.
- The proposed method of this paper is different from using simple or non-physiological data (such as accelerometer and GPS) to determine training load [4,5]. This paper proposes a number of physiological data to measure physical fitness which could understand the subject’s fatigue and prevent injuries in real time.
- The Rating of Perceived Exertion (RPE) allows participants to use their own feelings during exercise (heartbeat, breathing, perspiration, muscle fatigue, etc.) to estimate the intensity of exercise. The PRE method must be evaluated after exercise, such as the Session-RPE method which is evaluated by the subject’s subjective judgment [6]. Therefore, it is different from the real-time monitoring and evaluation method proposed in this paper.
The wearable device consists of many sensors such as accelerometer, hear rate sensor, blood pressure sensors, etc. The accelerometer sensors can help the user to count steps or estimate daily energy. However, the accelerometer sensors have low accuracy at low velocity [7,8] and if the user is in an emergency situation, the accelerometer sensors cannot detect the danger as a physical signal. All commercial wearable devices have adopted the accelerometer sensor as the major measuring physical signal sensors, so that they cannot provide efficient data in an emergency situation. The most significant physical emergency situation is always with cardiovascular risk. If the wearable device can detect the cardiovascular risk factor [9], it is important for trainer to avoid unnecessary training. The factors of cardiovascular risk, such as monitoring heart rate or blood pressure, can help to predict the abnormal cardiovascular statement. Moreover, the body temperature of the trainer is also an important factor to measure health. Therefore, our study wants to focus on heart rate and temperature to design a wearable device detecting the trainer’s physiological state to prevent an abnormal situation.
This paper proposes an evaluation method of the physical fitness, which uses physiological information such as risk factors, body temperature, heart rate, and blood oxygen concentration to evaluate physical fitness. The evaluated value of the physical fitness is a comprehensive evaluation value of physiological information, so it has no direct correlation with the medical/training needs of the solution.
- Everyone can get an evaluation value of physical fitness through this system, and there is no limit to the special users. The experimental results of this paper are used to prove that during exercise, the evaluation value of physical fitness reacts to the actual physical fitness changes.
- The evaluation value of physical fitness is a response to the change in real physical fitness. It can be seen from the experimental results that the physical fitness changes before, during, and after exercise are indeed correctly reflected in the evaluation value of physical fitness.
- This system is connected to the user’s mobile phone via WiFi, and connected to the Internet via the 4G network in the user’s mobile phone. Therefore, users can save their exercise process data as long as they have a 4G network.
This system is connected to the user’s mobile phone via WiFi, and connected to the Internet via the 4G network in the user’s mobile phone. Therefore, users can save their exercise process data as long as they have a 4G network. On the other hand, our system adopted the fuzzy theory that consists of two stages: prediction and update. We predict the heart rate if the signal loss occurs in the system, and it will alarm automatically in prediction mode. These functions can support the trainer in an emergency situation. The training environment does not always have good network quality, owing to cellular base station disappearance, so the off-line communication function can support the transmit message without cellular signal. Because the signal will be lost, the heart rate must be predicted to avoid a dangerous situation. We also surveyed wearable devices for mountaineering activity, studied over five years as shown in Table 1. Reference [10] suggested a cloud-based emergency response and SOS system for trainers when they encounter danger. Reference [11] proposed a trainer-assisted wearable device and emergency rescue system architecture which comprises a wearable device. Reference [12] presented an in-ear pulse oximeter mountaineering system for continuous measurement of vital signs. These mountaineering wearable devices did not have off-line communication mode and health prediction.
The hardware of this paper is the prototype of the product. According to current technology, it is not difficult to commercialize the hardware, and the power supply part can also be reduced considerably.
Available wearable devices can be designed for the integration of various physiological factors in training and are suitable for interactive applications among many people. Thus, the research design of this study is based on Mobile Edge Computing [13] and Communication (MECC). The main purpose of the proposed fitness training device is to effectively assist trainers with physical fitness training, including a real-time understanding of a trainee’s physiological state and potential injury risk based on the intensity of the training and environmental factors. When an abnormality is detected, the device will immediately warn the trainer and provide diagnostic and environmental information so that trainers can observe the status of all players at any time or those of immediate medical interest. This study constructs a communication network for the proposed device, using a 4G mobile network connecting servers to the cloud and sorting through the data in a cloud server. Therefore, a trainer can have access to the medical status of all players on a team in real-time during any training session. This network is achieved by utilizing fuzzy theory to show the physiological state of trainees. The main purpose of this device is to effectively support the trainer in managing the intensity of a player’s fitness training by monitoring the risk factor, body temperature, heart rate, and blood oxygen levels, including environmental factors.
2. Related Works
The system proposed integrates a wearable device and the MECC. This section will discuss related literature and describe the development of today’s wearable devices.
There are many types of wearable devices, including glasses type, watch type, wearable type, etc., and currently mainstream commercialized products are mainly smart watches and smart bracelets. The purpose of a smart bracelet is similar to that of a smart watch. It mainly focuses on collecting health information, such as recording calories burned, walking or running distance, recording sleep status, etc., or with reminding functions such as alarm clock, time, weather, and finding mobile phones. In addition to the above-mentioned functions, the smart watch also has diversified functions such as calling, photographing, recording, and mobile payment. As smart watches require low power consumption and compact appearance, smart watches usually emphasize the battery, panel and sensing functions, so the price is usually more expensive.
Whether watches or bracelets, what kind of benefits do these wearable devices provide to people’s lives? The main demands of such mobile devices are nothing more than health protection and medical care. From the perspective of wearable devices, there are already smart bracelets, watches, etc. that demand personal independent health management. There are also some auxiliary medical devices designed for medical and nursing needs, which are usually used in telemedicine and remote monitoring. Doctors can track the patient’s condition and patients can be treated at home and are assisted in their early recovery.
It is understood that the wearable devices currently used in medical treatment include implantable wearable medical devices such as brain nerve stimulators, gastric stimulators, cardiac defibrillators/electric shock devices, insulin syringes, etc.; there are also wearable devices such as personal emergency rescue devices such as pedometer, health bracelet, wearable defibrillator, and OK bounce chest/heart rate monitoring patch, etc.
It is worth observing that consumer-grade products, such as smart watches and health bracelets are quite popular now. They are mostly used by professional or amateur athletes, office workers in leisure and fitness, etc., and they are still personally independent in use. Health management uses Edge computing and Big data as a platform for Wearable IoT data analysis, and can provide knowledge solutions to several wearable device issues [14,15]. We have provided a comprehensive survey and classification of commercially available wearables and research prototypes.
- Wearable Device
A wearable device is simple and easy to use, has low power consumption, and miniaturizes its basic functions. It can be worn on the body, offering wearers convenient features and interaction, in addition to the benefits of network applications equipment [16]. Wearable devices can be worn daily with little to no inconvenience, further embedding and integrating wearable technology into people’s lives [17,18].
- Mobile Edge Computing and Communication
The MECC is known as the third wave of the information revolution, following computers and the Internet. It was first proposed in 2009 by Kevin Ashton, director of the Massachusetts Institute of Technology’s Auto-ID Center [19]. “Things” refer to connected devices, including firmware, communication devices, and information platforms relating to connected devices [20]. Things generally connect via a wireless network because MECC may contain 500 megabytes of objects. Devices monitoring a person’s physiological state can connect to the Internet, monitoring a user’s environment through the MECC. The proposed system can be centrally managed and controlled. The goal of the MECC is to enable everything around us to access the Internet or connect via wireless remote terminals and link all future smart items, including furniture, cars, appliances, and so on. All things can transmit data and be controlled over the Internet [21].
The present study proposes an MECC wearable device system. The device can monitor the physiological state of the human body. It measures individual heart rate, body temperature, blood oxygen concentration, and risk factor in the environment and can determine the most suitable training intensity for an individual. The sensor can monitor each individual state, and measures the body’s tolerance by using fuzzy theorem. This chapter introduces the measurement methods.
- Risk Factor Index
Risk factor is determined according to the Second Military General Hospital and the National Army Education and Training Service Implementation Guidelines [22]. We have survived studies between health and body temperature [23,24,25,26,27]. Typically, the circadian rhythm can be detected by the body temperature [23,24]. Furthermore, the body temperature rhythm can also be noticed with health problems like breathlessness [25]. Therefore, we can observe the body temperature rhythm to detect the breathlessness situation, and our system can also detect body temperature without detecting the breathing rate. Heart rate managing heart output is a major element in thermoregulation. Therefore, heart rate measurements influence metabolic rate [27]. By measuring changes in temperature and humidity in the environment, risk factor determines the possible impact on the human body in the current environment. The measurement formula is “outdoor temperature (°C) + outdoor relative humidity (%) × 0.1,” and the calculated coefficient is divided into safe (<30), attention (30–35), warning (35–40), and danger (>40). During exercise, the human body temperature will rise. If the ambient temperature is the same as the body temperature, dissipating heat will be almost impossible. Therefore, the ambient temperature is most comfortable below the body temperature. If heat cannot be dissipated, the body will be uncomfortable. According to research, the most comfortable sports environment temperature is 24–26 °C, and the best performance environment temperature is 26 °C. Therefore, it is important that the risk factor posed by environmental temperature is clearly understood. Table 2 illustrates the risk factor measurement method and the preventative measures to be taken for each state.
- Body Temperature
Body temperature refers to the internal temperature of the human body. The average normal body temperature is approximately 35.4–37.4 °C. Body temperature is kept constant by temperature regulation, which is controlled by the hypothalamus. However, many factors affect body temperature, such as day–night cycle, age, disease, and movement at the time. Excessive body temperature can lead to organ failure and lesions, leading to local fatigue [28]. Generally speaking, body temperature will gradually rise when exercising, and the degree of the body temperature ascent is related to the intensity of training. If the heat regulating mechanisms fail or immediate cooling is not possible, the body temperature will rise beyond a safe level. A body core temperature above 40 °C is considered dangerous overheating [3] as shown in Table 3. This temperature rise is the result of muscles producing more heat than sweat, with blood flow dissipating. The heat generated during strenuous exercise is 15–20 times that of the body at rest. If no heat dissipates, then the body temperature can be increased by 1 °C every 5 min. Sustained overheating can cause heat exhaustion. If timely cooling is not provided, the situation will be life-threatening and will have a high mortality rate. Table 2 shows the possible effects of body temperature on the human body (for example, adult male and female).
- Heart Rate
Heart rate may reflect stimulation by body movement. Maximum heart rate is an appropriate indicator of exercise intensity. The average heart rate is calculated as shown in the following formula, and the average heartbeat of a person is important. However, heart rate can increase as a result of long-term exercise in the training process [3], and is affected by age and resting heart rate. The most common heartbeat sensors [29] today are the hand-clip and ear-clip types. In the proposed device design, the ear-clip type is more suitable. Thus, this study uses an ear-clip heart-rate sensor to measure the heart rate of the subject, as shown in Figure 1. Most commercial wearable devices for measuring HR/HRV require the user to rest and wait for one minute to generate the HR signal. However, the ear clip sensor does not need the user to rest and it can detect HR signal immediately. For our proposed system, it is easy to cause undetectable conditions, so we chose to use the ear clip sensor.
The heart rate is measured first when a wearer is at rest. Through the heart-rate calculation, factors like age or physical state can be eliminated [3]. Then, the physical state of a player can be correctly determined using heart rate. This indicator can help make appropriate training adjustments, including rest and balance for the current training intensity [3].
- Step 1: 220 − age = maximum heart rate
- Step 2: Reserve heart rate = maximum heart rate − resting heart rate
- Step 3: Target heart rate = resting heart rate + (reserve heart rate × exercise level)
Subjects of different ages have different heartbeat indicators, and exceeding the heartbeat indicated for a specific age is dangerous. Table 4 shows the heartbeat index and the highest safe-heart rate for persons aged 20–70 years old.
Heart rate is the most easily acquired physiological information. When heart rate is monitored during exercise, it can reflect the strengths and weaknesses of cardio-respiratory function [30]. During exercise, the heart rate can be improved according to a range of indicators, such as age. A heart-rate target range should be 75% of the body’s highest heart rate. Age is also an important heartbeat indicator. This factor is related to monitoring a subject’s evaluated physiological condition, and the general center jump is between 50% and 80%, as shown in Figure 2.
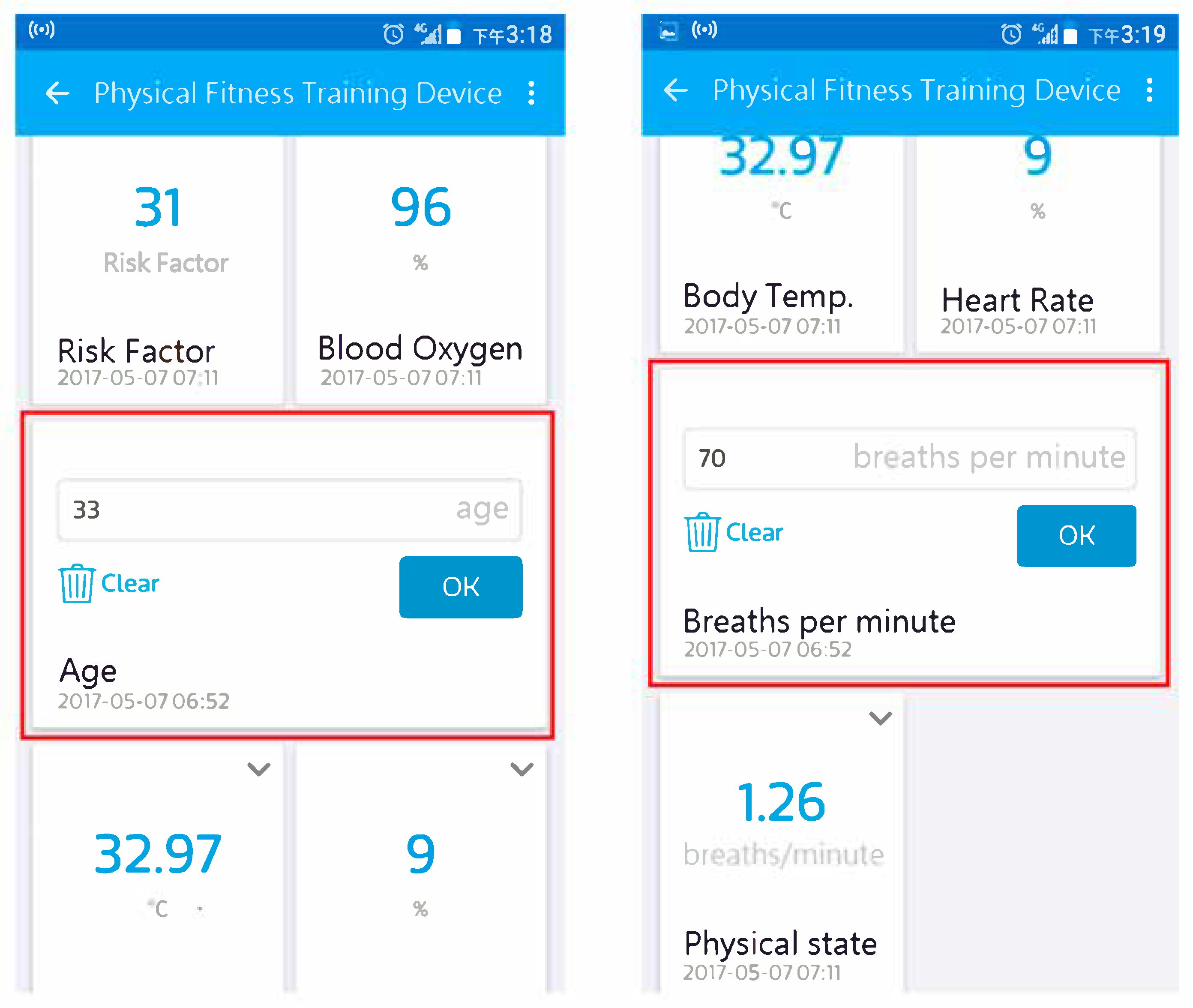
A user first enters the MediaTek Cloud Sandbox (MCS) platform to pre-enter their age and resting heart rate. The user presses a button on the proposed device to obtain their current health status. Using the heart-rate calculation, different ages or physical states can be excluded. The system can then correctly determine the physical status of the user.
The physical fitness index proposed in this paper will be calculated and evaluated on the device and sent back to the cloud server via the Internet. Therefore, when the system has poor network connectivity, the system can still use HR predictions to evaluate physical fitness index, but on-board computing is still required.
- Blood Oxygen Concentration
The human body requires oxygen to function, and the circulatory system ensures that blood carrying oxygen is carried to each part of the body. Blood oxygen concentration (SpO2) refers to the amount of oxygen bound to hemoglobin (HbO2) in the blood as a percentage of capacity. The body acquires oxygen via the respiratory system, and monitors the oxygen carrying capacity of hemoglobin (Hb) in the blood [32,33,34,35,36]. Oxygen saturation should generally be no less than 94%, as SpO2 < 90% indicates a state of hypoxemia, that is, a standard tissue cell metabolism in hypoxic state. A severe hypoxic condition (SpO2 < 80%) can cause lactic acid buildup, indicative of insufficient mitochondrial oxygenation. The resulting decrease in synthesis of ATP produces myocardial depression leading to bradycardia. Organs, such as the brain and heart, may be damaged as a result. The SpO2 value can be regarded as an important indicator of ventricular fibrillation arrhythmia and cardiac arrest [37]. SpO2 is the percentage of oxygen saturation or amount in the blood. The amount of oxygen in the blood tends to remain relatively stable even during exercise and sleep. Generally speaking, the blood oxygen concentration of a normal person should be kept above 94% (95–100%). If it is below 94%, clinically appropriate oxygen will be given to maintain sufficient blood oxygen concentration. Special attention should be paid. If the blood oxygen is lower than 90%, seek medical attention is as soon as possible. The reason why SpO2 is used in this paper is that the sensors currently on the market are relatively easy to obtain.
3. The Proposed Method: Physical Fitness Training Device
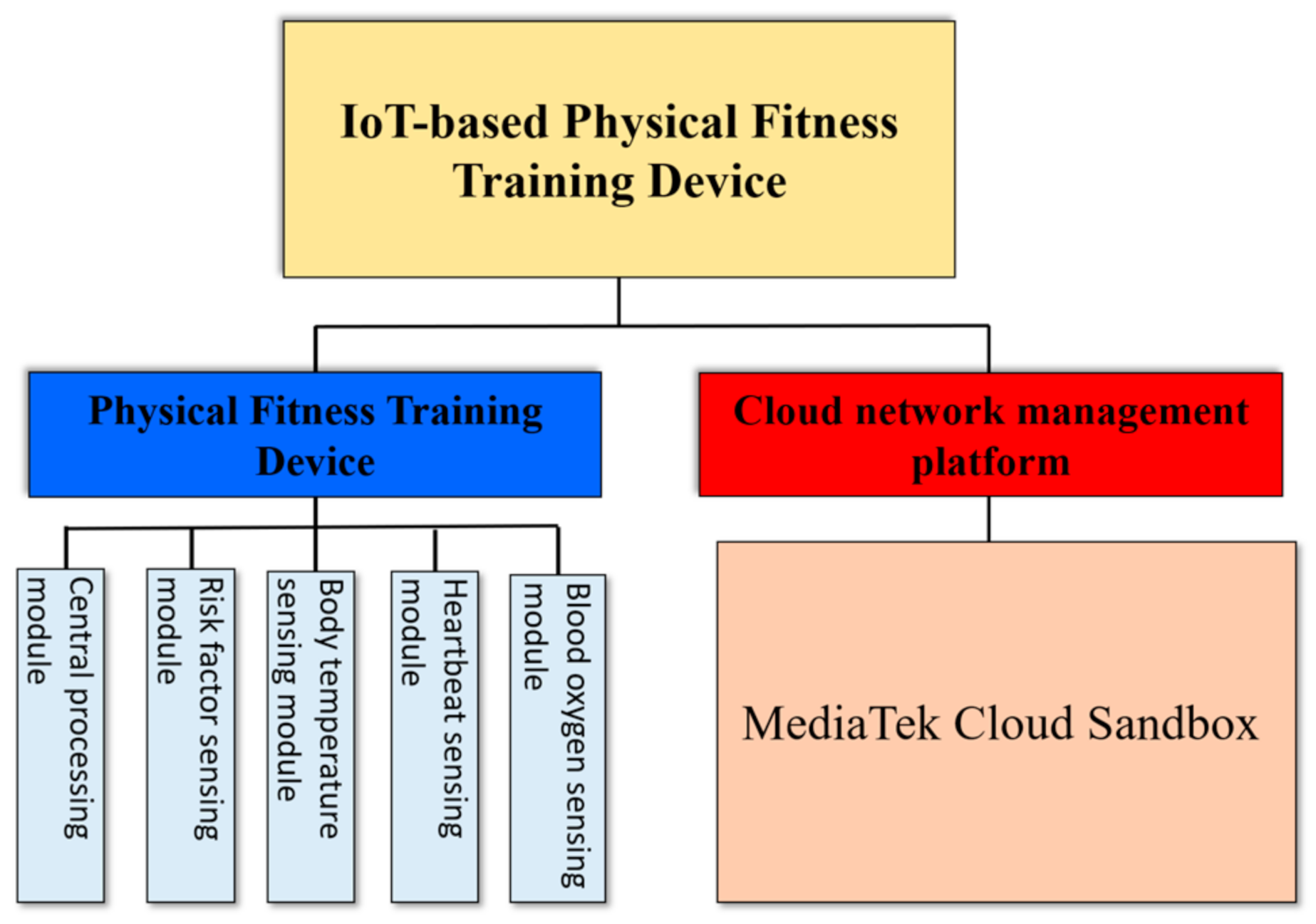
The physical fitness training management device developed in this research includes a physical fitness training management and cloud network management platform. Figure 3 shows the architecture of the device. The physical fitness training management aspect is mainly responsible for measurement. The sensed physiological data is uploaded to the cloud using the 4G network management platform. The fitness management device consists of a central processing module and sensing modules, such as a temperature sensing module, a risk factor module, and a heartbeat sensing module, as shown in Figure 4. The central processing module is responsible for receiving the temperature data from the sensing module, sensing the heartbeat information, and measuring the risk factor. The device then uses a radio transmission module to upload the data to the cloud network management platform. When the device determines that the test subject is in an abnormal condition, a warning signal and notification will be sent by the cloud management system to the trainer and wearer. This paper proposes to use the IoT to return user physical indicators. Since the 5G “Internet of Things” technology is not yet mature, we propose a method of transmission via the 4G network of the mobile phone. The reason why the mobile phone is not returned is that when the 5G technology matures in the future, this device can operate independently without a mobile phone. On the other hand, under multi-person management, it is more suitable to return data to the server for integrated management.
This device only measures and evaluates physical fitness data in objective view, and does not discuss physical and/or mental stress in response to changing exercise conditions. Excessive physical training can cause coma or shock. We hope to avoid such situations through this device. Although there are some wearable devices already available in the market can monitor the wearer’s body temperature and can send appropriate notifications. However, none of these devices can integrate the measured information and give a physical fitness index, which is also one of the most important contributions of this paper. Physical fitness index is when the body’s ability to adapt to the external environment can be regarded as the body’s comprehensive ability to adapt to life, exercise, and the environment (for example, temperature, climate change or viruses, etc.). It contains two aspects, general quality (the state of physical health) and specific quality (specific physical abilities required to perform a certain occupation or sport). In addition to being competent for daily work, there is also spare time to enjoy leisure, and the physical fitness and ability to cope with sudden changes and stress. Therefore, good physical fitness usually requires correct balanced nutrition, exercise, diet management, and adequate sleep and rest.
- Central Processing Module
This study used a LinkIt Smart 7688 Duo development platform as the central processing module. This platform was designed mainly for networking wearable devices. The chip used had 32 MB of flash memory and 128 MB of DDR2 RAM. The chip’s pin design and the expansion board are easy to integrate directly into a product. This study used the Arduino IDE platform, and uploads were performed using the 7688 LinkIt Smart platform.
The MediaTek LinkIt ™ Smart 7688 Duo is powered by the OpenWrt Linux and a 580 MHz MIPS processor and is with an ATMega32U4 Arduino microcontroller. With on-board WiFi support, this device truly provides everything needed to quickly prototype IoT devices and applications all on one small and affordable board. We used this device to implement our system prototype and the firmware coding is easy to build in other embedded kits. Its advantage is that it has a built-in wifi module to facilitate the development of IoT related applications.
This chip uses an MT7688AN wireless chipset with an ATmega32U4 microcontroller (MCU). The MT7688AN system-level chip is the core of the development platform. Moreover, this system-level chip has high performance 802.11n 1T1R Wi-Fi AP, supports up to 2 GB of RAM, and includes an SD card. It has a Wi-Fi encryption engine and various peripheral connection capabilities. Developers can also use the UART interface to communicate with the MCU, as shown in Figure 5.
- Body Temperature Sensing Module
This study used an MLX90614 module to measure a subject’s body temperature. The Melexis MLX90614 is a non-contact infrared thermometer for temperature measurement with an IR thermopile detector chip. The digital output of the thermometer is PWM. In the 10-bit PWM configuration, the continuous output measurement range is between −20 °C and 120 °C. In addition, the MLX90614 has a low-noise amplifier and a powerful DSP unit for high precision and thermometer resolution. The temperature of the environment is calculated accurately.
- Risk Factor Sensing Module
This study uses a DHT11 temperature and humidity sensor to monitor external temperature and humidity for risk factor assessment. It can collect real-time humidity and temperature data. The sensors’ simple single-chip computer bus can be used to communicate directly through the calibrated digital signal output. The DHT11 uses minimal power, and the average operating current is 0.5 mA. Upon receiving a start signal, the DH11T response signal is received by the Arduino system platform, with a delay of 20–40 µs.
- Blood Oxygen Sensing Module
This study uses an ear-clip type MAX30100 pulse oximetry sensor. The MAX30100 sensor is a pulse oximeter heart-rate sensor. In general, this device is an optical sensor whose measured readings come from the two LEDs emitting two wavelengths of light. The emitted light is focused on a permeable single point to monitor the oxygenated blood in the skin.
- Cloud Network Management Platform [38]
MCS is a free cloud-based platform, which allows fast prototyping of wearable devices for data and device management services, focusing mainly on MECC connectivity. MCS is presented in webpage form and provides the MCS APP for Android and iOS. It can collect its own API data returned from the device and provide a graphical interface to display data in the development of the page. A developer can create a prototype by collecting the information using the MCS from the sensing elements of the device. These data channels can be divided into the following categories: display, controller, and integrated display controller. This type of data channel and display can store and display the data collected by the sensing elements of the device. For example, data on temperature are uploaded from the sensing component of the device, and the MCS will store the data in a time series by monitoring the situation in real time. The MCS can also control the remote terminal through the webpage. The device uses a built-in controller system to control the state of the components within the device.
The MCS can set trigger conditions and actions. When the value returned by a specific data channel exceeds the set range, the system will send an email or mobile phone notification. Users can also choose whether to receive email or mobile phone notifications. MCS supports webhook trigger, and it can enter the URL notification made. The system will set automatic notifications when a specific condition is triggered (push phone or email), and the notification will be sent to each user. Thus, trainers can be immediately notified according to the set trigger conditions, and implement timely training adjustments or medical treatment for risk management and prevention. Figure 6 shows the MCS operating interface.
The MCS can also perform multi-person management. The multi-person management interface can be operated by IDs of different devices, and multiple devices can be monitored at the same time. The MCS can also control a remote terminal through the controls in the webpage. The use of the built-in system handover command to the controller has a long buzzer sound in long or short tones. This command allows operation management, as shown in Figure 7.
4. Proposed Fuzzy Theory
This study used the fuzzy inference engine to make inferences to determine appropriate decisions. The fuzzy rule of this experiment was extracted from the measurement data. The membership function parameters measured the amount of collected data to fine-tune the membership function. These factors include the risk factor, individual body temperature, heart rate, and blood oxygen fuzzy sets. The fuzzy rules can be linked to infer the values of the test subject indicators, and the index coefficient is understood by the present physiological state of the test subject. According to reference [21], we determined the degree of risk and training benefits, as shown in Figure 8.
- Fuzzy Theory Algorithm
Fuzzy logic systems have been widely applied in many fields of scientific and academic research on MECC devices, such as, washing machines, air-conditioners, and refrigerators. The fuzzy system can support smart control to automatically fine-tune temperature, humidity, or mechanical action. Fuzzy theory provides a logic system to deal with human logical inference processes and can design intelligent systems to analyze semantics or descriptive language. In the past few years, fuzzy deduction has been widely applied to various practical systems [39]. Most applications have been in consumer goods or industrial intelligent control systems and use the rules of experience or knowledge-related information and fuzzy control law. The propositional linguistic control is transformed into the if–then rule form [40].
However, most inference usually follows the method presented in [41]. Inference methods have advantages and disadvantages, and this study uses a Min–Max inference method. The inference of fuzzy inference result is obtained by quantization. By monitoring the data collected and then inputting fuzzy rules to obtain the calculation result, the degree of motion of the subject or the current state of the body can be determined.
- Fuzzy Rule Establishment
The fuzzy inference method in this study is the attribution function to obtain the appropriate degree of each rule. The appropriateness of each rule is integrated to achieve appropriate deduction. Even if the propositions in the rule conditions are not completely consistent, they can be compared according to the level of consistency. The reasoning process is performed in the following four steps: (1) fuzzification of the input variables, (2) rule evaluation, (3) output of the aggregation rule, (4) and final inverse fuzzification [42].
The fuzzy inference method consists of determining the appropriateness of using the membership function for each rule, and then integrating all the rules of fitness to obtain the proper inference. Experiment outputs include the risk factor, individual temperature, heart rate, and oxygen saturation (SpO2). Four input/output systems are decomposed into a number of input/output systems. The fuzzy rules are based on 54 kinds of (3 × 3 × 3 × 2) composition state. The fuzzy rules may be reduced to nine kinds of semantic fuzzy rule.
In summary, the inference engine in the fuzzy system will use these fuzzy rules to make inferences to determine the decision to be taken in the next step. The fuzzy rules of this experiment are extracted from the measured data by the physical training algorithm. The attribution function is collected by the data. The parameters of the attribution function are fine-tuned, such as the fuzzy coefficient, temperature, heart rate, and blood oxygen. The fuzzy set can be associated with the fuzzy rule, and the fuzzy rule base inference is measured, as shown in Figure 9.
Physiological states have four sets: E1 (safe), E2 (sports), E3 (dangerous), and E4 (prohibited), as shown in Figure 9.
In this experiment, the numerical range of each device for monitoring the fitness exercise management device system contains fuzzy sets. The range of the risk factor is A1 (safe, 0–30), A2 (notification, 27–39), and A3 (dangerous, 40–60). This study adopted the normal fuzzy normalization, taking the range of 1–0 as 26–30. A value of 1 is 100%, and 0 is 0%. For example, the risk factor input value X1 is measured as 29, then the attribution degree of A1 and A2 is 0.4 and 0.6, respectively. Figure 10 shows the attribution coefficient obtained after the input of the risk factor.
Next, the membership function range of body temperature, heart rate, and blood oxygen were measured. First, body temperature can safely be between about 35.4 and 37.4 °C. If it is more than 40 °C, then the subject must stop exercising and seek medical attention. This study uses the set values for normal temperature as B1 (26–30 °C), moderate temperature as B2 (27–39 °C), and high temperature as B3 (above 40 °C). Figure 11 shows a domain of the temperature membership function set.
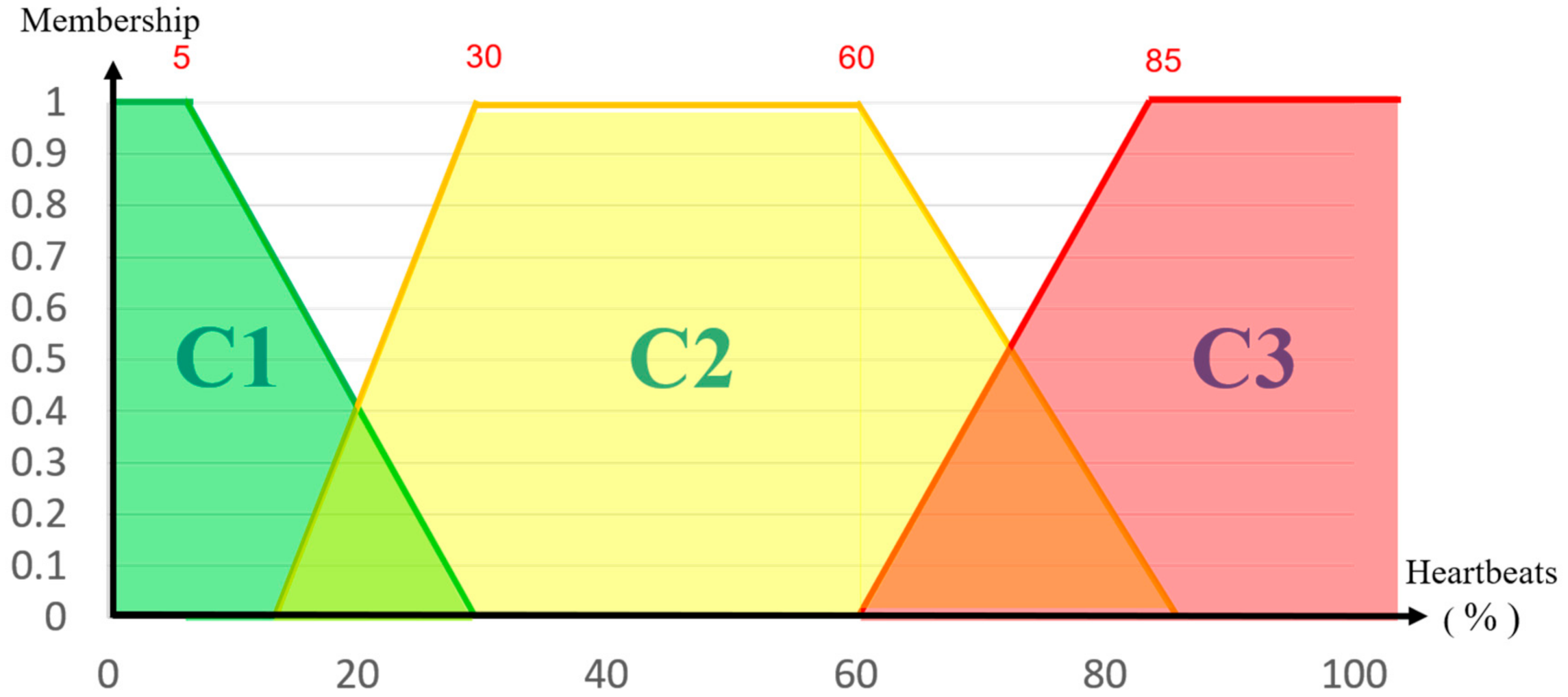
Heart rate is usually measured as the number of times the heart beats in 1 min. Heart rate is automatically calculated by inputting the age and resting heart rate into the proposed system. The heart rate is approximately 50–80% during general exercise. This rate involves minimal sweating, and subjects are conscious of slightly heavier breathing. Thus, the system calculates normal heart rate as C1 (20–40%), moderate as C2 (40–79%), and excessive as C3 (80–100%), as shown in Figure 12.
Pulse oximetry (SpO2) is considered abnormal if it is lower than a 94% oxygen saturation. An SpO2 of less than 80% indicates severe hypoxia. This condition causes subendocardial lactic acid accumulation by decreasing synthesis of ATP. When resulting in myocardial depression, it will lead to bradycardia, which can cause ventricular fibrillation arrhythmia and even cardiac arrest [43]. Thus, the attribution function values are defined as dangerous D1 (SpO2 ≤ 90%) and normal D2 (SpO2 = 91–100%). If blood oxygen falls below 90%, then the system will send a warning signal to the trainer to stop the exercise. Figure 13 shows the blood oxygen input.
The system has four variables, namely, risk coefficient, body temperature, heart rate, and blood oxygen. The fuzzy sets can be related to the fuzzy rules, and the physiological state of the measured person is inferred by the fuzzy rule of the latter term. The final output of the fuzzy system must be a clear value. The input of the inverse fuzzy process is the output of the aggregated fuzzy set. The output is a single value. This study uses the most common centroid method. This method lies along the vertical line of the polymerization divided into two equal parts: the centroid of gravity (COG) of the mathematical equation [20], as follows:
5. Experimental Result
The proposed device was further equipped with a commercial power supply, a LED light, a warning buzzer, and an oxygen concentration sensor, as shown in Figure 14.
The test environment was a 3000 m run. The testing user was a 33-year-old adult man with a resting heart rate of 70 beats/min. The experiment explored the benefits of the device in a practical environment. First, the user entered his resting heart rate and age on the cloud platform, as shown in Figure 15.
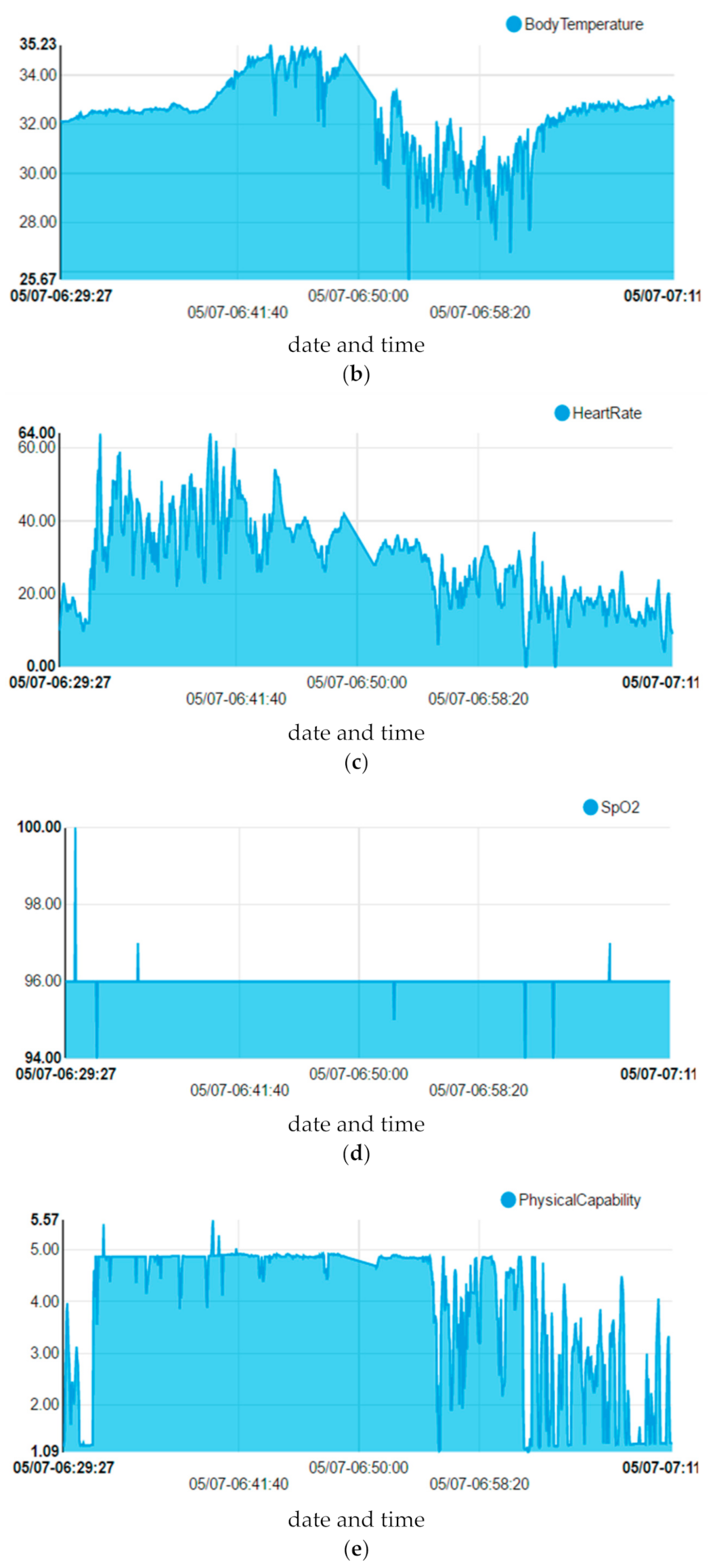
The respective risk factor, body temperature, heart rate, and SpO2 sensing data were summarized, and the physical state of the subject was shown, as in Figure 16. It can be seen from the Figure 16d that exercise has no obvious effect on the change of blood oxygen value. The reason is that the change of blood oxygen value must be under high-intensity continuous exercise to have a chance to change drastically. Figure 17 shows a complete exercise cycle, and the changes in the first, middle, and late stages of exercise can be seen from the changes in physical fitness index.
When we collect experimental data, we also record the physiological responses of the subjects. When designing the membership functions of the fuzzy theory, we use manual to fine-tune the results close to the true reflections, so as to determine the membership function of the fuzzy theory.
The actual machine test has four sensors, and this study used fuzzy calculus to determine the physical indicators during exercise, as shown in Figure 17. From the analysis of the monitoring records and comparison with different values, the subject is at rest before 1.09, whereas he is in an exercise state from 4.0–5.57. This result is a reasonable scope of movement. The degree of exercise loading can be found in the degree of difference between rest and exercise. The subsequent gradual recovery will slow the heartbeat and lower body temperature more than the recovery. The slow walk from the value of the running state is obvious. The physical fitness indicators vary with the development of different sport states.
Figure 16d shows that exercise has no obvious effect on the change of blood oxygen value. The reason is that the change of blood oxygen value must be under high-intensity continuous exercise to have a chance to change drastically. We obtain real-time actual data from the sensor, and calculate the risk factor through the chip, as shown in Figure 16. The respective sensing data from Figure 16 used fuzzy calculus to determine the physical indicators in Figure 17. The acquisition and calculation of this information is done in real time on the device.
The fuzzy output value is defined as the physical fitness index. In the case of this experiment, the present physical index was determined using the values measured by the proposed device. Table 5 shows the results of the physical fitness management device measuring the physical fitness index, and the analyzed results obtained during exercise.
In order to test the differences in physical index between different ages, we found three subjects of different age groups to test the stability of physical fitness indicators. The 20-person experiment refers to the test of the mountain environment and verifies to the accuracy of the system. We first tested our system by three users, their ages are 24, 45, and 62. The age ranges are youth, middle age, and old age and for fair testing comparison, they were tested under 3000 m in the same environment—the results are shown in the Table 6. Our proposed system with three other testers were under resting heart rates of 68, 75, and 70 beats/min, respectively. The average physical index of the experiment result is 5.6. Table 7 shows their physical index.
The experiment indicated that the proposed system satisfied its purpose and function demands of the initial studies and was able to monitor the physiological state of the test subject and the exercise intensity through the wearable device. For example, if the exercise intensity was between 5 and 6, a trainer could choose different modes of exercise or time to manage a subject’s physical status to achieve effective exercise.
Our system was tested by the 20 users. These users are autonomous in mountaineering without any “controlled”, in order to reflect the most real data. The 20 users’ ages are between 18–30. The testing environment of the mountain (Taiwu Mountain of Quemoy) is a total of 253 m, and each user’s exercise time is 90 min. The average errors in heart rate and body temperature are 1.7 and 0 °C, respectively. We also adopted the statistical hypothesis testing for evaluating our testing data. First, we utilized the variance analysis to test if the variance is different or not. The p-value of homogeneity of variance is 0.546, and it is larger than 0.05. It is defined as no significant difference. Then, we also did the two-sample t-test based on equal variance to test mean value difference. After doing the two-sample t-test, the p-value was 0.426 and larger than 0.05. Therefore, there is no significant difference. However, the average heart rate error is 1.7, but our system is stable according to statistical hypothesis testing shown in Table 7. In this paper, the data of the subjects collected at the beginning is used to establish the membership functions of the fuzzy theory. When designing the membership functions of the fuzzy theory, we use manual to fine-tune the results close to the true reflections, so as to determine the membership function of the fuzzy theory. In order to test the differences in physical index between different ages, we found three subjects of different age groups to test the stability of physical fitness indicators. The 20-person experiment refers to the test of the mountain environment and verifies to the accuracy of the system. In the system test, these subjects are autonomous in mountaineering without any “controlled”, in order to reflect the most real data. This device is designed to integrate the physical fitness data of the subject and propose a physical fitness index for evaluation. The information shared regarding safe HR and HR target range do not need to be discussed in this paper. On the other hand, the membership functions of fuzzy theory will also convert HR into a corresponding membership value.
We have used smart watch and smart phone for synchronization validation, but some sensors will differ due to different wearing positions, but they do not affect the calculation results of relative physical indicators.
6. Conclusions
The health benefits of exercise are unquestionable, but training accidents or injuries are unavoidable. More than 90% of sport-related deaths are caused by heart or respiratory problems, or heatstroke. Many athletes experience fatigue during strenuous exercise, which can cause myocardial hypoxia and sudden death. In fact, any exercise that reaches a certain intensity may cause heart problems, especially in those who have cardiovascular diseases. Unfortunately, most people who die while exercising are unaware of their heart-related problems. If such problems are identified early, then the chances of severe injury or death during exercise can be reduced.
Heart rate estimation with a low-cost device is a popular research application. The use of pulse HR monitoring during physical exercise is difficult, because the accurate heart rate measurement by the heart rate motion artifacts (MAs) is hard to achieve. The pulse heart rate is embedded with a low-cost heart rate device. Nevertheless, it is difficult to measure the presence of motion artifacts in monitoring during physical exercise. We proposed a predicted approach denoising the HR measurement smoothly. Our study can improve better accuracy in terms of heart rate estimation. Therefore, the novelty of our system is to adopt the fuzzy theory to predict heart rate more accurately with a low-cost heart rate device. From experimental results obtained in this study, the human body was found to have its own timely warnings for imminent injury during exercise, such as fatigue. Moreover, new technology allows the instantaneous interaction of wearable devices and network cloud systems. Hence, this technology makes monitoring a subject during exercise for any warning signs of imminent injury possible, allowing trainers or users to make appropriate adjustments to their exercise and offering accurate physiological data so that timely treatment can be applied in the case of an injury. The proposed device monitors the risk factor, heartbeat, blood oxygen level, and body temperature in the environment, and uses fuzzy theory to calculate the various states of the human body. However, the authors believe that future work should explore connecting the device to home monitoring and medical system applications. The human body is extremely complex, and future work should include other factors to be monitored, such as blood pressure, blood sugar, and GPS. This research is aimed at broadening the scope of applications and functions offered by wearable medical messaging systems.
Author Contributions
Y.-X.Z., Z.-X.L. and Y.-Z.H.; methodology, Z.-X.L.; software, Y.-X.Z.; validation, Y.-X.Z.; formal analysis, Y.-Z.H.; investigation, Y.-X.Z.; resources, Z.-X.L.; data curation, Z.-X.L. and Y.-Z.H.; writing—original draft preparation, Y.-X.Z. and Y.-Z.H.; writing—review and editing, S.-S.L.; funding acquisition, P.-Y.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was partly supported by the University System of Taipei Joint Research Program (contracts USTP-NTUT-NTOU-109-01, USTP-NTOU-TMU-108-01 and USTP-NTUT-NTOU-108-04), and Ministry of Science and Technology, Taiwan, under grants MOST-110-2221-E-019-051-, MOST-109-2622-E-019-010-, MOST-109-2221-E-019-057-, MOST-110-2634-F-019-001-, MOST-110-2634-F-008-005- and MOST-110-2221-E-019-052-MY3, MOST-108-2221-E-019-038-MY2, MOST-110-2218-E-002-032-MBK.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jones, B.H.; Cowan, D.N.; Knapik, J.J. Exercise, training and injuries. Sports Med. 1994, 18, 202–214. [Google Scholar] [CrossRef] [PubMed]
- Murakami, H.; Kawakami, R.; Nakae, S.; Yamada, Y.; Nakata, Y.; Ohkawara, K.; Sasai, H.; Ishikawa-Takata, K.; Tanaka, S.; Miyachi, M. Accuracy of 12 wearable devices for estimating physical activity energy expenditure using a metabolic chamber and the doubly labeled water method: Validation study. JMIR mHealth uHealth 2019, 7, e13938. [Google Scholar] [CrossRef]
- Galli, A.; Narduzzi, C.; Giorgi, G. Measuring heart rate during physical exercise by subspace decomposition and kalman smoothing. IEEE Trans. Instrum. Meas. 2017, 67, 1102–1110. [Google Scholar] [CrossRef]
- Halson, S.L. Monitoring training load to understand fatigue in athletes. Sports Med. 2014, 44, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, R.; Brito, J.P.; Martins, A.; Mendes, B.; Marinho, D.A.; Ferraz, R.; Marques, M.C. In-season internal and external training load quantification of an elite European soccer team. PLoS ONE 2019, 14, e0209393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, M.; Stylianides, G.; Djaoui, L.; Dellal, A.; Chamari, K. Session-RPE method for training load monitoring: Validity, usefulness, and influencing factors. Front. Neurosci. 2017, 11, 612. [Google Scholar] [CrossRef]
- Tophøj, K.H.; Petersen, M.G.; Sæbye, C.; Baad-Hansen, T.; Wagner, S. Validity and reliability evaluation of four commercial activity trackers’ step counting performance. Telemed. e-Health 2018, 24, 669–677. [Google Scholar] [CrossRef]
- Svarre, F.R.; Jensen, M.M.; Nielsen, J.; Villumsen, M. The validity of activity trackers is affected by walking speed: The criterion validity of Garmin Vivosmart® HR and StepWatch™ 3 for measuring steps at various walking speeds under controlled conditions. PeerJ 2020, 8, e9381. [Google Scholar] [CrossRef]
- World Health Organization. World Health Statistics 2020: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Chen, C.-M.; Li, C.-T.; Liu, S.; Wu, T.-Y.; Pan, J.-S. A provable secure private data delegation scheme for mountaineering events in emergency system. IEEE Access 2017, 5, 3410–3422. [Google Scholar] [CrossRef]
- Lee, S.-H.; Ni, J.-C.; Zhao, Y.-G.; Yang, C.-S. A real-time emergency rescue assistance system for mountaineers. In Proceedings of the 2017 IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 8–10 January 2017; pp. 106–107. [Google Scholar] [CrossRef]
- Venema, B.; Leonhardt, S. In-ear pulse oximetry in high altitude mountaineering. In Proceedings of the 13th IASTED International Conference on Biomedical Engineering (BioMed), Innsbruck, Austria, 20–21 February 2017; pp. 254–259. [Google Scholar] [CrossRef]
- Mao, Y.; You, C.; Zhang, J.; Huang, K.; Letaief, K.B. A survey on mobile edge computing: The Communication perspective. IEEE Commun. Surv. Tutorials 2017, 19, 2322–2358. [Google Scholar] [CrossRef] [Green Version]
- Poongodi, T.; Krishnamurthi, R.; Indrakumari, R.; Suresh, P.; Balusamy, B. Wearable devices and IoT. In A Handbook of Internet of Things in Biomedical and Cyber Physical System; Balas, V., Solanki, V., Kumar, R., Ahad, M., Eds.; Springer: Cham, Switzerland, 2002; Volume 165. [Google Scholar] [CrossRef]
- Seneviratne, S.; Hu, Y.; Nguyen, T.; Lan, G.; Khalifa, S.; Thilakarathna, K.; Hassan, M.; Seneviratne, A. A survey of wearable devices and challenges. IEEE Commun. Surv. Tutor. 2017, 19, 2573–2620. [Google Scholar] [CrossRef]
- Bariya, M.; Nyein, H.Y.Y.; Javey, A. Wearable sweat sensors. Nat. Electron. 2018, 1, 160–171. [Google Scholar] [CrossRef]
- Seshadri, D.R.; Craker, J.; Rowbottom, J.R.; Voos, J.E.; Drummond, C. Wearable devices for sports: New integrated technologies allow coaches, physicians, and trainers to better understand the physical demands of athletes in real time. IEEE Pulse 2017, 8, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Swetha, P.; Zhu, Y. Nanomaterial-enabled wearable sensors for healthcare. Adv. Health Mater. 2018, 7, 1700889. [Google Scholar] [CrossRef]
- Ashton, K. That ‘Internet of Things’ thing. RFID J. 2009, 22, 97–114. [Google Scholar]
- Abolfazli, S.; Sanaei, Z.; Ahmad, E.; Gani, A.; Buyya, R. Cloud-based augmentation for mobile devices: Motivation taxonomies and open challenges. IEEE Commun. Surveys Tuts 2013, 16, 337–368. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Wolter, K. Stochastic analysis of delayed mobile offloading in heterogeneous networks. IEEE Trans. Mob. Comput. 2018, 17, 461–474. [Google Scholar] [CrossRef]
- Phegley, J.; Perkins, K.; Gupta, L.; Dorsey, J.K. Risk factor fusion for predicting multifactorial diseases. IEEE Trans. Biomed. Eng. 2002, 49, 72–76. [Google Scholar] [CrossRef]
- Benloucif, S.; Guico, M.J.; Reid, K.J.; Wolfe, L.F.; L’Hermite-Balériaux, M.; Zee, P.C. Stability of melatonin and temperature as circadian phase markers and their relation to sleep times in humans. J. Biol. Rhythm. 2005, 20, 178–188. [Google Scholar] [CrossRef] [Green Version]
- Bos, S.C.; Waterhouse, J.; Edwards, B.; Simons, R.; Reilly, T. The use of actimetry to assess changes to the rest-activity cycle. Chrono-Biol. Int. 2003, 20, 1039–1059. [Google Scholar]
- Dauch, W.A.; Bauer, S. Circadian rhythms in the body temperatures of intensive care patients with brain lesions. J. Neurol. Neurosurg. Psychiatry 1990, 53, 345–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikitopoulou, G.; Crammer, J.L. Change in diurnal temperature rhythm in manic-depressive illness. BMJ 1976, 1, 1311–1314. [Google Scholar] [CrossRef] [Green Version]
- Berglund, L.G. Heart rate as an indicator of metabolic rate in hot environments. In Proceedings of the 30th Annual Conference on Engineering in Medicine and Biology, Los Angeles, CA, USA, 5–9 November 1977; p. 274. [Google Scholar]
- Brooks, G.A.; Fahey, T.D. Exercise Physiology: Human Bioenergetics and Its Applications; Macmillan: New York, NY, USA, 1984. [Google Scholar]
- Nelson, B.W.; Low, C.A.; Jacobson, N.; Areán, P.; Torous, J.; Allen, N.B. Guidelines for wrist-worn consumer wearable assessment of heart rate in biobehavioral research. NPJ Digit. Med. 2020, 3, 90. [Google Scholar] [CrossRef]
- Munje, R.D.; Muthukumar, S.; Prasad, S. Lancet-free and label-free diagnostics of glucose in sweat using Zinc Oxide based flexible bioelectronics. Sens. Actuators B Chem. 2017, 238, 482–490. [Google Scholar] [CrossRef]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices Évid. Res. 2014, 7, 231–239. [Google Scholar] [CrossRef]
- Walker, E.J.; McAinch, A.J.; Sweeting, A.; Aughey, R.J.; Information, P.E.K.F.C. Inertial sensors to estimate the energy expenditure of team-sport athletes. J. Sci. Med. Sport 2016, 19, 177–181. [Google Scholar] [CrossRef]
- Micklewright, D.; Gibson, A.S.C.; Gladwell, V.; Al Salman, A. Development and validity of the rating-of-fatigue scale. Sports Med. 2017, 47, 2375–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMartini, J.K.; Martschinske, J.L.; Casa, D.J.; Lopez, R.M.; Ganio, M.S.; Walz, S.M.; Coris, E.E. Physical demands of National Collegiate Athletic Association Division I football players during preseason training in the heat. J. Strength Cond. Res. 2011, 25, 2935–2943. [Google Scholar] [CrossRef] [PubMed]
- Enoka, R.M.; Duchateau, J. Muscle fatigue: What, why and how it influences muscle function. J. Physiol. 2008, 586, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Yoo, S.K. Motion artifact reduction in photoplethysmography using independent component analysis. IEEE Trans. Biomed. Eng. 2006, 53, 566–568. [Google Scholar] [CrossRef]
- Laptook, A.R.; Salhab, W.; Allen, J.; Saha, S.; Walsh, M. Pulse oximetry in very low birth weight infants: Can oxygen saturation be maintained in the desired range? J. Perinatol. 2006, 26, 337–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MediaTek Cloud Sandbox. Available online: http://labs.mediatek.com/en/platform/mediatek-cloud-sandbox (accessed on 1 June 2021).
- Eyoh, I.; John, R.; De Maere, G. Interval type-2 A-intuitionistic fuzzy logic for regression problems. IEEE Trans. Fuzzy Syst. 2018, 26, 2396–2408. [Google Scholar] [CrossRef]
- Wu, C.; Liu, J.; Jing, X.; Li, H.; Wu, L. Adaptive fuzzy control for nonlinear networked control systems. IEEE Trans. Syst. Man, Cybern. Syst. 2017, 47, 2420–2430. [Google Scholar] [CrossRef]
- Mendel, J. Fuzzy logic systems for engineering: A tutorial. Proc. IEEE 1995, 83, 345–377. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.C. Fuzzy logic in control systems: Fuzzy logic controller—Part I and part II. IEEE Trans. Syst. Man Cybern. 1990, 20, 404–435. [Google Scholar] [CrossRef] [Green Version]
- Zadeh, L.A. Fuzzy sets. Inf. Control. 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Ear-clip heart-rate sensor.

Figure 2.
Effect of training on heart rate [31].
Figure 2.
Effect of training on heart rate [31].

Figure 3.
Architecture of the proposed device.

Figure 4.
Fitness management device schematic.

Figure 5.
LinkIt Smart 7688 Duo Support Program List.

Figure 6.
MCS system interface.

Figure 7.
MCS multiplayer management interface.

Figure 8.
Fuzzy rules.

Figure 9.
Diagram of fuzzy rules.

Figure 10.
Coefficient of the fuzzy sets.

Figure 11.
Fuzzy set domain of body temperature.

Figure 12.
Fuzzy set of heart rate.

Figure 13.
Set for blood oxygenation.

Figure 14.
Fitness training machine model management system.

Figure 15.
Heart rate and age of the subject.

Figure 16.
Respective sensing data: (a) risk factor, (b) body temperature, (c) heart rate, (d) SpO2, (e) physical indicators.
Figure 16.
Respective sensing data: (a) risk factor, (b) body temperature, (c) heart rate, (d) SpO2, (e) physical indicators.


Figure 17.
Physical indicator monitoring records.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The commercial wearable devices.
| Heart Rate | Temperature | Emergency Call | With Smartphone | Off-Line Communication Mode | Health Prediction | |
|---|---|---|---|---|---|---|
| [10] | True | True | True | True | False | False |
| [11] | True | True | True | True | False | False |
| [12] | True | False | False | False | False | False |
| Our system | True | True | True | False | True | True |
Table 2.
Risk factor index for body and external temperature [3].
Table 2.
Risk factor index for body and external temperature [3].
| Heatstroke Risk Factor Measurement Method | ||
|---|---|---|
| Risk Factor | Situation | Prevention Focus |
| <30 | Safety | Normal daily routine |
| 30–35 | Note | Water supplement |
| 35–40 | Warning | Water supplement and avoid intense sports |
| >40 | Adjustment | Change clothing or location |
Table 3.
Effect of body temperature on the human body [3].
Table 3.
Effect of body temperature on the human body [3].
| Body Temperature (°C) | Human Body State | Possible Danger |
|---|---|---|
| 35–37.4 | Normal body temperature | No |
| 37.4–39.5 | Exercise or fever | Fatigue, vasodilation |
| 40–42 | Heat dissipation is out of regulation, body is overheated | Overheating causes rapid breakdown of proteins, leading to death |
Table 4.
Safe heart-rate indicators and maximum heart rates for persons aged 20–70 years old.
| Age | Safe Heart-Rate Indicators | Maximum Heart Rate |
|---|---|---|
| 20 | 100–150/min | 200/min |
| 25 | 98–146/min | 195/min |
| 30 | 95–142/min | 190/min |
| 35 | 93–138/min | 185/min |
| 40 | 90–135/min | 180/min |
| 45 | 88–131/min | 175/min |
| 50 | 85–127/min | 170/min |
| 55 | 83–123/min | 165/min |
| 60 | 80–120/min | 160/min |
| 65 | 78–116/min | 155/min |
| 70 | 75–113/min | 150/min |
Table 5.
Physical fitness status table.
| Physical Index | State of the Human Body |
|---|---|
| 0–1.9 | Safe state |
| 2.0–3.5 | Walking, warm-up exercise |
| 3.6–4.5 | Cycling, early jogging, feeling hot |
| 4.6–5.4 | Sweating, gasping, discomfort |
| 5.5–6.8 | Running for more than 10 min, profuse sweating, fatigue |
| 6.9–7.9 | Sprinting, weightlifting, shortness of breath, mild muscle soreness |
| 8–8.7 | Difficulty in breathing, chest tightness, high body temperature, inability to perspire |
| 8.9–10 | Heat phlegm, heart disease, organ failure |
Table 6.
Three testers’ experiment result.
| Tester | Years Old | Resting Heart Rate | Physical Index |
|---|---|---|---|
| 1 | 24 | 68 | 5.2 |
| 2 | 45 | 75 | 5.8 |
| 3 | 62 | 70 | 6 |
Table 7.
Experiment results of 20 users.
| Testers | Evaluated Heart Rate | Real Heart Rate | Evaluated Body Temperature (°C) | Real Body Temperature (°C) |
|---|---|---|---|---|
| User 1 | 121 | 115 | 36.6 | 36.6 |
| User 2 | 130 | 125 | 36.5 | 36.5 |
| User 3 | 114 | 113 | 36.6 | 36.6 |
| User 4 | 118 | 120 | 36.6 | 36.6 |
| User 5 | 130 | 118 | 36.4 | 36.4 |
| User 6 | 105 | 112 | 36.6 | 36.6 |
| User 7 | 125 | 119 | 36.2 | 36.2 |
| User 8 | 109 | 110 | 36.2 | 36.2 |
| User 9 | 116 | 119 | 36.4 | 36.4 |
| User 10 | 128 | 115 | 36.4 | 36.4 |
| User 11 | 115 | 111 | 36.7 | 36.7 |
| User 12 | 112 | 109 | 36.4 | 36.4 |
| User 13 | 125 | 128 | 36.7 | 36.7 |
| User 14 | 120 | 122 | 36.7 | 36.7 |
| User 15 | 126 | 124 | 36.5 | 36.5 |
| User 16 | 118 | 115 | 36.4 | 36.4 |
| User 17 | 117 | 119 | 36.5 | 36.5 |
| User 18 | 129 | 132 | 36.6 | 36.6 |
| User 19 | 125 | 122 | 36.5 | 36.5 |
| User 20 | 123 | 124 | 36.6 | 36.6 |
| p-value of homogeneity of variance | 0.546 | 1 | ||
| Two sample t-test | 0.426 | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zhao, Y.-X.; Lu, Z.-X.; Hsieh, Y.-Z.; Lin, S.-S.; Chiang, P.-Y. The Wearable Physical Fitness Training Device Based on Fuzzy Theory. Appl. Sci. 2021, 11, 9976. https://0-doi-org.brum.beds.ac.uk/10.3390/app11219976
AMA Style
Zhao Y-X, Lu Z-X, Hsieh Y-Z, Lin S-S, Chiang P-Y. The Wearable Physical Fitness Training Device Based on Fuzzy Theory. Applied Sciences. 2021; 11(21):9976. https://0-doi-org.brum.beds.ac.uk/10.3390/app11219976
Chicago/Turabian StyleZhao, Yu-Xiang, Zheng-Xian Lu, Yi-Zeng Hsieh, Shih-Syun Lin, and Pei-Ying Chiang. 2021. "The Wearable Physical Fitness Training Device Based on Fuzzy Theory" Applied Sciences 11, no. 21: 9976. https://0-doi-org.brum.beds.ac.uk/10.3390/app11219976
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.