
FDG PET/CT versus Bone Marrow Biopsy for Diagnosis of Bone Marrow Involvement in Non-Hodgkin Lymphoma: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.2.1. Inclusion Criteria
- Studies that analyse [18F]FDG PET/CT’s role in diagnosing BMI in comparison to the invasive BMB for NHL patients.
- Studies carried out for NHL patients.
- Studies published in English.
- Studies published until 1 November 2021.
2.2.2. Exclusion Criteria
- Studies that did not involve comparison between the [18F]FDG-PET/CT and BMB.
- Studies that contain only BMB test, or only [18F]FDG-PET/CT exam.
- Studies carried out only for Hodgkin lymphoma patients.
- Studies that include previously diagnosed patients with NHL.
- Studies that did not assess the BMI.
- Studies that did not differentiate between the previously treated patients and HL patients from NHL-diagnosed patients.
- Studies published only as abstracts.
- Case reports, review articles, recommendations, letters, conference abstracts.
- Studies conducted on animals.
2.3. Study Quality
2.4. Data Extraction
3. Results
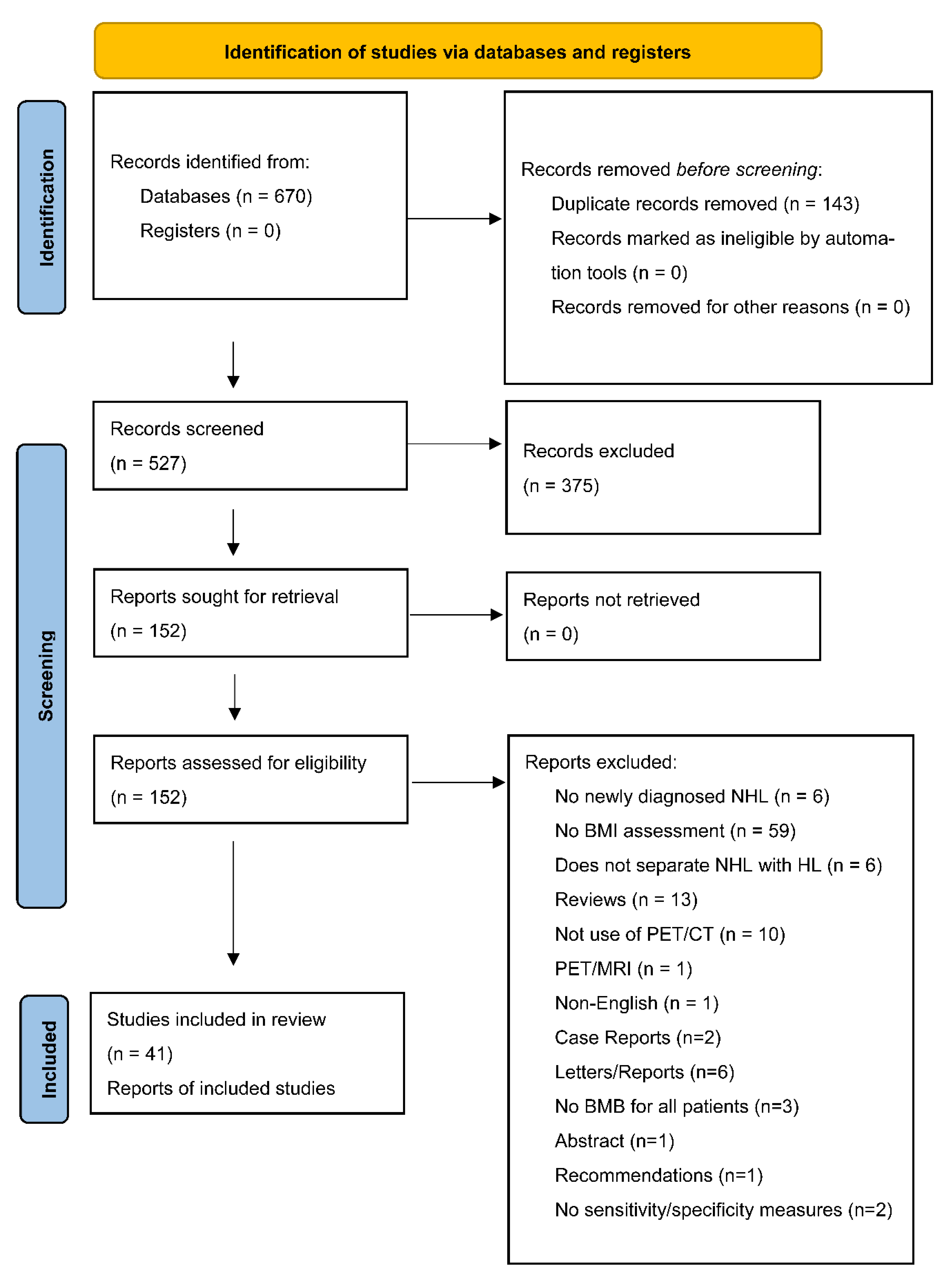
3.1. Search Results
3.2. Characteristics of the Included Studies
3.3. Methodological Quality Assesment
3.4. Diagnostic Performance of PET/CT and BMB in Determining BMI
3.4.1. Diagnostic Performance of [18F]FDG PET/CT and BMB in Determining BMI in NHL Patients
3.4.2. Diagnostic Performance of [18F]FDG PET/CT and BMB in Determining BMI in Subtypes Lymphoma
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Ekberg, S.E.; Smedby, K.; Glimelius, I.; Nilsson-Ehle, H.; Goldkuhl, C.; Lewerin, C.; Jerkeman, M.; Eloranta, S. Trends in the prevalence, incidence and survival of non-Hodgkin lymphoma subtypes during the 21st century—A Swedish lymphoma register study. Br. J. Haematol. 2020, 189, 1083–1092. [Google Scholar] [CrossRef]
- Thandra, K.C.; Barsouk, A.; Saginala, K.; Padala, S.A.; Barsouk, A.; Rawla, P. Epidemiology of Non-Hodgkin’s Lymphoma. Med. Sci. 2021, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Li, D.; Hu, G.; Huang, Q.; Wang, P.; Cai, J. Diagnostic performance of 18F-FDG PET/CT in pediatric lymphoma infiltrating bone marrow: A meta-analysis. Clin. Transl. Imaging 2021, 9, 511–522. [Google Scholar] [CrossRef]
- Susanibar-Adaniya, S.; Barta, S.K. Update on Diffuse large B cell lymphoma: A review of current data and potential applications on risk stratification and management. Am. J. Hematol. 2021, 96, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Park, B.B.; Jeong, J.Y.; Kim, W.Y.; Jang, S.; Shin, B.K.; Lee, D.S.; Han, J.H.; Park, C.J.; Suh, C.; et al. Assessment of bone marrow involvement in patients with lymphoma: Report on a consensus meeting of the Korean Society of Hematology Lymphoma Working Party. Korean J. Intern. Med. 2016, 31, 1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, J.; Lee, Y.; Park, Y.; Kim, S.G.; Hwang, K.H.; Park, S.H.; Jeong, J.; Kim, K.H.; Ahn, J.Y.; Park, S.; et al. Role of FDG-PET/CT in detecting lymphomatous bone marrow involvement in patients with newly diagnosed diffuse large B-cell lymphoma. Ann. Hematol. 2012, 91, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Kim, J.Y.; Ahn, H.K.; Lee, S.M.; Sym, S.J.; Park, J.; Cho, E.K.; Ahn, J.Y.; Park, S.; Lee, S.P.; et al. Bone marrow involvement is predictive of infusion-related reaction during rituximab administration in patients with B cell lymphoma. Supportive Care Cancer 2013, 21, 1145–1152. [Google Scholar] [CrossRef]
- Lister, T.A.; Crowther, D.; Sutcliffe, S.B.; Glatstein, E.; Canellos, G.P.; Young, R.C.; Rosenberg, S.A.; Coltman, C.A.; Tubiana, M. Report of a committee convened to discuss the evaluation and staging of patients with Hodgkin’s disease: Cotswolds Meeting. J. Clin. Oncol. 1989, 7, 1630–1636. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059. [Google Scholar] [CrossRef]
- Adams, H.J.; Kwee, T.C.; de Keizer, B.; Fijnheer, R.; de Klerk, J.M.; Nievelstein, R.A. FDG PET/CT for the detection of bone marrow involvement in diffuse large B-cell lymphoma: Systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.K.; Yeh, C.L.; Tsui, C.C.; Liang, J.A.; Chen, J.H.; Kao, C.H. F-18 FDG PET for evaluation of bone marrow involvement in non-Hodgkin lymphoma: A meta-analysis. Clin. Nucl. Med. 2011, 36, 553–559. [Google Scholar] [CrossRef]
- Weiler-Sagie, M.; Bushelev, O.; Epelbaum, R.; Dann, E.J.; Haim, N.; Avivi, I.; Ben-Barak, A.; Ben-Arie, Y.; Bar-Shalom, R.; Israel, O. 18F-FDG avidity in lymphoma readdressed: A study of 766 patients. J. Nucl. Med. 2010, 51, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pakos, E.E.; Fotopoulos, A.D.; Ioannidis, J.P. 18F-FDG PET for evaluation of bone marrow infiltration in staging of lymphoma: A meta-analysis. J. Nucl. Med. 2005, 46, 958–963. [Google Scholar]
- Aguado-Vázquez, T.M.; Olivas-Martínez, A.; Cancino-Ramos, U.; Zúüiga-Tamayo, D.A.; Lome-Maldonado, M.D.C.; Rivas-Vera, S.; García-Pérez, F.O.; Candelaria-Hernández, M.G. 18f-Fluorodeoxyglucose Positron Emission Tomography Versus Bone Marrow Biopsy for the Evaluation of Bone Marrow Infiltration in Newly Diagnosed Lymphoma Patients. Rev. Investig. Clin. 2021, 73, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Kaddu Mulindwa, D.; Altmann, B.; Held, G.; Angel, S.; Stilgenbauer, S.; Thurner, L.; Bewarder, M.; Schwier, M.; Pfreundschuh, M.; Löffler, M.; et al. FDG PET/CT to detect bone marrow involvement in the initial staging of patients with aggressive non-Hodgkin lymphoma: Results from the prospective, multicenter PETAL and OPTIMAL >60 trials. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3550–3559. [Google Scholar] [CrossRef]
- Göçer, M.; Kurtoğlu, E. Comparison of Bone Marrow Involvement with Bone Marrow Biopsy and PET–CT and Evaluation of Any Effects on Survival in Patients Diagnosed with Hodgkin and Non-Hodgkin Lymphoma. Indian J. Hematol. Blood Transfus. 2021, 37, 52–59. [Google Scholar] [CrossRef]
- Maisarah, S.; Mahayuddin, A.M.; Fadzilah, H. Assessing bone marrow involvement in diffuse large B-cell lymphoma with 18F-FDG PET/CT: A preliminary experience at Hospital Pulau Pinang. Med. J. Malays. 2021, 76, 665–671. [Google Scholar]
- Lim, C.H.; Hyun, S.H.; Cho, Y.S.; Choi, J.Y.; Lee, K.H. Prognostic significance of bone marrow 2-[18F]Fluoro-2-deoxy-d-glucose uptake in diffuse large B-cell lymphoma: Relation to iliac crest biopsy results. Clin. Radiol. 2021, 76, 550.e19–550.e28. [Google Scholar] [CrossRef]
- Nakajima, R.; Moskowitz, A.J.; Michaud, L.; Mauguen, A.; Batlevi, C.L.; Dogan, A.; Schöder, H. Baseline FDG-PET/CT detects bone marrow involvement in follicular lymphoma and provides relevant prognostic information. Blood Adv. 2020, 4, 1812–1823. [Google Scholar] [CrossRef]
- St-Pierre, F.; Broski, S.M.; LaPlant, B.R.; Maurer, M.J.; Ristow, K.; Thanarajasingam, G.; Macon, W.R.; Habermann, T.M.; Witzig, T.E. Fluorodeoxyglucose-Positron Emission Tomography Predicts Bone Marrow Involvement in the Staging of Follicular Lymphoma. Oncologist 2020, 25, 689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Sabbagh, A.; Ibrahim, F.; Szabados, L.; Soliman, D.S.; Taha, R.Y.; Fernyhough, L.J. The Role of Integrated Positron Emission Tomography/Computed Tomography (PET/CT) and Bone Marrow Examination in Staging Large B-Cell Lymphoma. Clin. Med. Insights Oncol. 2020, 14, 1179554920953091. [Google Scholar] [CrossRef]
- Kandeel, A.A.; Hussein, M.; Zidan, L.; Younis, J.; Edesa, W.; Alsayed, Y. Diagnostic performance of 18F-2-fluoro-2-deoxy-D-glucose PET/computerized tomography in identifying bone marrow infiltration in new patients with diffuse large B-cell lymphoma and Hodgkin lymphoma. Nucl. Med. Commun. 2020, 41, 269–279. [Google Scholar] [CrossRef]
- Kupik, O.; Akin, S.; Tuncel, M.; Eren, G.; Türker, A.; Kars, A.; Erbaş, B. Comparison of clinical and PET-derived prognostic factors in patients with non-Hodgkin lymphoma: A special emphasis on bone marrow involvement. Nucl. Med. Commun. 2020, 41, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Elamir, Y.; Elazab, M.; Owis, A.S.; Elsayed, H.F. PET/CT and bone marrow biopsy (BMB) in evaluating bone marrow in lymphoma. Egypt. J. Radiol. Nucl. Med. 2020, 51, 201. [Google Scholar] [CrossRef]
- Büyükşimşek, M.; Kolsuz, İ.; Yetişir, A.E.; Tohumcuoğlu, M.; Oğul, A.; Mirili, C.; Paydaş, S.; Güney, İ.B. Performance of Positron Emission Tomography-Computed Tomography and Bone Marrow Biopsy in Detecting Bone Marrow Infiltration in Lymphoma Cases. Turk. J. Hematol. 2020, 37, 220. [Google Scholar] [CrossRef]
- Tezol, Ö.; Sağcan, F.; Özcan, P.P.; Çıtak, E.Ç. Bone marrow involvement in pediatric malignancies: A comparison study of Positron emission tomography-computed tomography and bone marrow biopsy. Turk. J. Pediatrics 2020, 62, 182–190. [Google Scholar] [CrossRef]
- Yang, S.; Fu, L.; AbuduRxiti, M.; Wu, J.; Wang, Q.; Qin, Y.; Zou, X.; Li, H. Application of 18F-fluorodeoxyglucose positron emission tomography/computerized tomography in mantle cell lymphoma. Nucl. Med. Commun. 2020, 41, 477–484. [Google Scholar] [CrossRef]
- Xiao-Xue, W.; Xinyue, H.; Lijun, Z. Whole body FDG-PET/CT for the assessment of bone marrow infiltration in patients with newly diagnosed lymphoma. Med.Clin. 2020, 154, 61–65. [Google Scholar] [CrossRef]
- Yağci-Küpeli, B.; Koçyiğit-Deveci, E.; Adamhasan, F.; Küpeli, S. The value of 18F-FDG PET/CT in detecting bone marrow involvement in childhood cancers. J. Pediatric Hematol./Oncol. 2019, 41, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; He, K.; Feng, F.; Wang, S.; Yin, Y.; Fu, H.; Wang, H. Metabolic tumor burden on baseline 18 F-FDG PET/CT improves risk stratification in pediatric patients with mature B-cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1830–1839. [Google Scholar] [CrossRef]
- Abe, Y.; Kitadate, A.; Usui, Y.; Narita, K.; Kobayashi, H.; Miura, D.; Takeuchi, M.; O’uchi, E.; O’uchi, T.; Matsue, K. Diagnostic and prognostic value of using 18F-FDG PET/CT for the evaluation of bone marrow involvement in peripheral T-cell lymphoma. Clin. Nucl. Med. 2019, 44, e336–e341. [Google Scholar] [CrossRef] [PubMed]
- Badr, S.; Kotb, M.; Elahmadawy, M.A.; Moustafa, H. Predictive value of FDG PET/CT versus bone marrow biopsy in pediatric lymphoma. Clin. Nucl. Med. 2018, 43, e428–e438. [Google Scholar] [CrossRef] [PubMed]
- Özpolat, H.T.; Yilmaz, E.; Goksoy, H.S.; Özpolat, S.; Dogan, Ö.; Unal, S.N.; Nalcaci, M. Detection of bone marrow involvement with FDG PET/CT in patients with newly diagnosed lymphoma. Blood Res. 2018, 53, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Wang, S.; He, K.; Ma, C.; Fu, H.; Wang, H. PET/CT predicts bone marrow involvement in pediatric non-Hodgkin lymphoma and may preclude the need for bone marrow biopsy in selected patients. Eur. Radiol. 2018, 28, 2942–2950. [Google Scholar] [CrossRef] [PubMed]
- Öner, A.O.; Budak, E.S.; Aydın, F.; Salim, O.; Yücel, O.K.; Akkaya, B.; Toptaş, T.; Boz, A.; Yıldız, A.; Güngör, F.; et al. Efficacy of 18F-2-fluoro-2-deoxy-D-glucose positron emission tomography/computerized tomography for bone marrow infiltration assessment in the initial staging of lymphoma. Mol. Imaging Radionucl. Ther. 2017, 26, 69. [Google Scholar] [CrossRef]
- Teagle, A.R.; Barton, H.; Charles-Edwards, E.; Dizdarevic, S.; Chevassut, T. Use of FDG PET/CT in identification of bone marrow involvement in diffuse large B cell lymphoma and follicular lymphoma: Comparison with iliac crest bone marrow biopsy. Acta Radiol. 2017, 58, 1476–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albano, D.; Patti, C.; Lagalla, R.; Midiri, M.; Galia, M. Whole-body MRI, FDG-PET/CT, and bone marrow biopsy, for the assessment of bone marrow involvement in patients with newly diagnosed lymphoma. J. Magn. Reson. Imaging 2017, 45, 1082–1089. [Google Scholar] [CrossRef]
- Pham, A.Q.; Broski, S.M.; Habermann, T.M.; Jevremovic, D.; Wiseman, G.A.; Feldman, A.L.; Maurer, M.J.; Ristow, K.M.; Witzig, T.E. Accuracy of 18-F FDG PET/CT to detect bone marrow clearance in patients with peripheral T-cell lymphoma–tissue remains the issue. Leuk. Lymphoma 2017, 58, 2342–2348. [Google Scholar] [CrossRef]
- El Karak, F.E.; Bou-Orm, I.R.; Ghosn, M.; Kattan, J.; Farhat, F.; Ibrahim, T.; Jreige, M.; Cheikh, J.E.; Haidar, M. PET/CT scanner and bone marrow biopsy in detection of bone marrow involvement in diffuse large B-cell lymphoma. PLoS ONE 2017, 12, e0170299. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, F.; Soyer, N.; Kiper, D.; Savaş, R.; Özsan, N.; Şahin, F.; Saydam, G.; Mahmut, T.Ö.B.Ü.; Tombuloğlu, M.; Özgür, Ö.M.Ü.R.; et al. The role of PET/CT in evaluation of bone marrow involvement in lymphoma patients at the initial staging. Marmara Med. J. 2017, 30, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Vishnu, P.; Wingerson, A.; Lee, M.; Mandelson, M.T.; Aboulafia, D.M. Utility of bone marrow biopsy and aspirate for staging of diffuse large B cell lymphoma in the era of positron emission tomography with 2-deoxy-2-[fluorine-18] fluoro-deoxyglucose integrated with computed tomography. Clin. Lymphoma Myeloma Leuk. 2017, 17, 631–636. [Google Scholar] [CrossRef]
- Alzahrani, M.; El-Galaly, T.C.; Hutchings, M.; Hansen, J.W.; Loft, A.; Johnsen, H.E.; Iyer, V.; Wilson, D.; Sehn, L.H.; Savage, K.J.; et al. The value of routine bone marrow biopsy in patients with diffuse large B-cell lymphoma staged with PET/CT: A Danish-Canadian study. Ann. Oncol. 2016, 27, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Chen-Liang, T.H.; Martin-Santos, T.; Jerez, A.; Senent, L.; Orero, M.T.; Remigia, M.J.; Muiña, B.; Romera, M.; Fernandez–Muñoz, H.; Raya, J.M.; et al. The role of bone marrow biopsy and FDG-PET/CT in identifying bone marrow infiltration in the initial diagnosis of high-grade non-Hodgkin B-cell lymphoma and Hodgkin lymphoma. accuracy in a multicenter series of 372 patients. Am. J. Hematol. 2015, 90, 686–690. [Google Scholar] [CrossRef]
- Kim, H.Y.; Kim, J.S.; Choi, D.R.; Kim, H.S.; Kwon, J.H.; Jang, G.D.; Kim, J.H.; Jung, J.Y.; Song, H.H.; Lee, Y.K.; et al. The clinical utility of FDG PET-CT in evaluation of bone marrow involvement by lymphoma. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2015, 47, 458. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.P.; Gill, H.; Wang, Y.; Kwong, Y.L.; Khong, P.L. Bone marrow uptake of indolent non-Hodgkin lymphoma on PET/CT with histopathological correlation. Nucl. Med. Commun. 2015, 36, 1035–1041. [Google Scholar] [CrossRef] [Green Version]
- Adams, H.J.; Kwee, T.C.; Fijnheer, R.; Dubois, S.V.; Nievelstein, R.A.; de Klerk, J.M. Direct comparison of visual and quantitative bone marrow FDG-PET/CT findings with bone marrow biopsy results in diffuse large B-cell lymphoma: Does bone marrow FDG-PET/CT live up to its promise? Acta Radiol. 2015, 56, 1230–1235. [Google Scholar] [CrossRef] [PubMed]
- Çetin, G.; Çıkrıkçıoğlu, M.A.; Özkan, T.; Karatoprak, C.; Ar, M.C.; Eşkazan, A.E.; Ayer, M.; Cerit, A.; Gözübenli, K.; Uysal, B.B.; et al. Can positron emission tomography and computed tomography be a substitute for bone marrow biopsy in detection of bone marrow involvement in patients with Hodgkin’s or non-Hodgkin’s lymphoma? Turk. J. Hematol. 2015, 32, 213. [Google Scholar] [CrossRef]
- Cortés-Romera, M.; Sabaté-Llobera, A.; Mercadal-Vilchez, S.; Climent-Esteller, F.; Serrano-Maestro, A.; Gámez-Cenzano, C.; González-Barca, E. Bone marrow evaluation in initial staging of lymphoma: 18F-FDG PET/CT versus bone marrow biopsy. Clin. Nucl. Med. 2014, 39, e46–e52. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.; Kwee, T.C.; Fijnheer, R.; Dubois, S.V.; Nievelstein, R.A.; de Klerk, J.M. Bone marrow 18F-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography cannot replace bone marrow biopsy in diffuse large B-cell lymphoma. Am. J. Hematol. 2014, 89, 726–731. [Google Scholar] [CrossRef]
- Adams, H.J.; Kwee, T.C.; Fijnheer, R.; Dubois, S.V.; Blase, P.E.; Nievelstein, R.A.; de Klerk, J.M. Utility of quantitative FDG-PET/CT for the detection of bone marrow involvement in follicular lymphoma: A histopathological correlation study. Skelet. Radiol. 2014, 43, 1231–1236. [Google Scholar] [CrossRef] [PubMed]
- Berthet, L.; Cochet, A.; Kanoun, S.; Berriolo-Riedinger, A.; Humbert, O.; Toubeau, M.; Dygai-Cochet, I.; Legouge, C.; Casasnovas, O.; Brunotte, F. In newly diagnosed diffuse large B-cell lymphoma, determination of bone marrow involvement with 18F-FDG PET/CT provides better diagnostic performance and prognostic stratification than does biopsy. J. Nucl. Med. 2013, 54, 1244–1250. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.B.; Barrington, S.F.; Mikhaeel, N.G.; Hunt, A.A.; Cameron, L.; Morris, T.; Carr, R. PET-CT staging of DLBCL accurately identifies and provides new insight into the clinical significance of bone marrow involvement. Blood 2013, 122, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Pelosi, E.; Penna, D.; Douroukas, A.; Bello, M.; Amati, A.; Arena, V.; Passera, R.; Bisi, G. Bone marrow disease detection with FDG-PET/CT and bone marrow biopsy during the staging of malignant lymphoma: Results from a large multi-centre study. Q. J. Nucl. Med. Mol. Imaging 2011, 55, 469. [Google Scholar] [PubMed]
- Mittal, B.R.; Manohar, K.; Malhotra, P.; Das, R.; Kashyap, R.; Bhattacharya, A.; Varma, N.; Varma, S. Can fluorodeoxyglucose positron emission tomography/computed tomography avoid negative iliac crest biopsies in evaluation of marrow involvement by lymphoma at time of initial staging? Leuk. Lymphoma 2011, 52, 2111–2116. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.M.; Chen, F.Y.; Jiang, X.X.; Gu, H.Y.; Yin, Y.; Xu, J.R. 18F-FDG PET, combined FDG-PET/CT and MRI for evaluation of bone marrow infiltration in staging of lymphoma: A systematic review and meta-analysis. Eur. J. Radiol. 2012, 81, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Tilly, H.; Da Silva, M.G.; Vitolo, U.; Jack, A.; Meignan, M.; Lopez-Guillermo, A.; Walewski, J.; André, M.; Johnson, P.W.; Pfreundschuh, M.; et al. Diffuse large B-cell lymphoma (DLBCL): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v116–v125. [Google Scholar] [CrossRef]
- Tsuchiya, J.; Yamamoto, M.; Bae, H.; Oshima, T.; Yoneyama, T.; Miura, O.; Tateishi, U. Tumor identification of less aggressive or indolent lymphoma with whole-body 11C-Acetate PET/CT. Clin. Nucl. Med. 2019, 44, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Freedman, A.; Jacobsen, E. Follicular lymphoma: 2020 update on diagnosis and management. Am. J. Hematol. 2020, 95, 316–327. [Google Scholar] [CrossRef] [Green Version]
- Mayerhoefer, M.E.; Riedl, C.C.; Kumar, A.; Dogan, A.; Gibbs, P.; Weber, M.; Staber, P.B.; Huicochea Castellanos, S.; Schöder, H. [18F] FDG-PET/CT radiomics for prediction of bone marrow involvement in mantle cell lymphoma: A retrospective study in 97 patients. Cancers 2020, 12, 1138. [Google Scholar] [CrossRef]
- Aide, N.; Talbot, M.; Fruchart, C.; Damaj, G.; Lasnon, C. Diagnostic and prognostic value of baseline FDG PET/CT skeletal textural features in diffuse large B cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 699–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurch, L.; Kluge, R.; Sabri, O.; Fischer, L.; Wendt, S.; Einsiedel, H.G.; Starke, S.; Kühl, J.S.; Christiansen, H.; Hirsch, F.W.; et al. Whole-body [18F]-FDG-PET/MRI for staging of pediatric non-Hodgkin lymphoma: First results from a single-center evaluation. EJNMMI Res. 2021, 11, 62. [Google Scholar] [CrossRef]
- Afaq, A.; Fraioli, F.; Sidhu, H.; Wan, S.; Punwani, S.; Chen, S.H.; Akin, O.; Linch, D.; Ardeshna, K.; Lambert, J.; et al. Comparison of PET/MRI with PET/CT in the evaluation of disease status in lymphoma. Clin. Nucl. Med. 2017, 42, e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, K.; Queiroz, M.; Huellner, M.W.; de Galiza Barbosa, F.; Buck, A.; Schaefer, N.; Stolzman, P.; Veit-Haibach, P. Diagnostic performance of FDG-PET/MRI and WB-DW-MRI in the evaluation of lymphoma: A prospective comparison to standard FDG-PET/CT. BMC Cancer 2015, 15, 1002. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Hernandez-Pampaloni, M.; Houseni, M.; Chamroonrat, W.; Basu, S.; Kumar, R.; Dadparvar, S.; Torigian, D.A.; Alavi, A. Age-related changes in the metabolic activity and distribution of the red marrow as demonstrated by 2-deoxy-2-[F-18] fluoro-D-glucose-positron emission tomography. Mol. Imaging Biol. 2007, 9, 300–307. [Google Scholar] [CrossRef]
- Aras, M.; Dede, F.; Ones, T.; Inanır, S.; Erdıl, T.Y.; Turoglu, H.T. Evaluation of physiological FDG uptake in the skeleton in adults: Is it uniformly distributed? Rev. Española Med. Nucl. Imagen Mol. 2014, 33, 286–289. [Google Scholar] [CrossRef]


{kind=link}
| No. | Search Term | Database Search Results | |
|---|---|---|---|
| PubMed | Scopus | ||
| #1 | non-Hodgkin OR non-Hodgkins OR PTCL OR Peripheral T-cell lymphoma OR MCL OR mantle cell lymphoma OR DLBCL OR diffuse large B-cell lymphoma OR FL OR Follicular lymphoma OR PMBCL OR Primary mediastinal large B-cell lymphoma OR BL OR Burkitt lymphoma | 101,834 | 193,114 |
| #2 | 2-fluoro-2-deoxy-D-glucose OR FDG OR Fluorodeoxyglucose OR PET/CT | 57,777 | 91,069 |
| #3 | biopsy | 323,619 | 840,810 |
| #4 | Bone marrow | 229,682 | 412,081 |
| #5 | #1 AND #2 AND #3 AND #4 | [Title/Abstract] 155 | [Title/Abstract/Keyword] 515 |
| Participants Details | PET/CT before or after | Interval between BMB & PET/CT | BMB Site | PET/CT Interpretation | Standard Reference Test | Ann Arbor Staging Patients No. | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author, Publication Year | Country | Pts | No. of Male & Female | Age (Years) | Age Range (Years) | Patient Recruitment | I | II | III | IV | |||||
| Aguado-Vázquez et al., 2021 [15] | Mexico | 297 | M 166 F 131 | 57 Median | Adult 43–66 | 2017–2018 | BT | NR | Unilateral | Qualit. | BMB | 31 | 51 | 46 | 169 |
| Kaddu-Mulindwa * et al., 2021 [16] | Germany | 930 | M 525 F 405 | 68 Median | Adult 18–80 | NR | NR | NR | NR | Qualit. | BMB | NR | NR | 501 | |
| Göçer et al., 2021 [17] | Turkey | 231 | M 138 F 93 | FL 60 DLBCL 58 Other 63.5 Median | Adult FL (32–85) DLBCL (18–86) Other (20–85) | 2010–2018 | BT | <15 days | Unilateral | Qualit. | BMB | FL 3 DLBCL 5 Other 2 | FL 5 DLBCL 42 Other 4 | FL 15 DLBCL 51 Other 10 | FL 23 DLBCL 29 Other 42 |
| Maisarah et al., 2021 [18] | Malaysian | 21 | M 13 F 8 | 45.6 Mean | Adult 18–80 | 2016–2018 | BT | <60 days | NR | Qualit./ Quant. | BMB | 2 | 6 | 5 | 8 |
| Lim et al., 2021 [19] | South Korea | 512 | M 283 F 229 | 57 Median | Adult 47–67 | 2009–2014 | BT | <7 days | Bilateral | Qualit. | BMB | 285 | 83 | 144 | |
| Nakajima et al., 2020 [20] | USA | 261 | M 135 F 126 | 58.1 Median | Adult 19.7–90.5 | 2002–2016 | BT | NR | NR | Qualit. | BMB | 70 | 24 | 47 | 120 |
| St-Pierre et al., 2020 [21] | USA | 548 | M 286 F 262 | 61 Median | Adult 19–91 | 2003–2016 | BT | NR | NR | Qualit./ Quant. | BMB | NR | NR | NR | NR |
| Al-Sabbagh et al., 2020 [22] | Qatar | 89 | M 64 F 25 | 48.6 Mean 48 Median | Adult 18–77 | 2003–2017 | BT | <30 days | Unilateral | Qualit. | BMB | 23 | 12 | 9 | 45 |
| Kandeel et al. 2020 [23] | Egypt | 88 | NR | NR | Adult | 2015–2018 | BT | <30 days | Unilateral | Qualit./ Quant. | BMB | NR | NR | NR | NR |
| Kupik et al., 2020 [24] | Turkey | 89 | M 55 F 34 | 54 Mean | Adult NR | 2011–2013 | BT | NR | NR | Qualit./ Quant. | BMB/Follow-up | NR | NR | NR | NR |
| Elamir * et al., 2020 [25] | Egypt | 57 | NR | NR | Adult NR | NR | BT | 2 weeks | NR | Qualit./ Quant. | BMB/Follow- up | NR | NR | NR | NR |
| Büyükşimşek et al., 2020 [26] | Turkey | 269 | M 159 F 110 | 52 Median | Adult 18–80 | 2011–2018 | BT | 2 weeks | Unilateral | Qualit. | NR | 45 | 58 | 101 | 65 |
| Tezol et al., 2020 [27] | Turkey | 20 | M 13 F 7 | 10.6 Mean | Pediatr. NR | 2008–2018 | BT | NR | Bilateral | Qualit./ Quant. | BMB | NR | NR | NR | NR |
| Yang et al., 2020 [28] | China | 39 | M 30 F 9 | 58.5 Mean | Adult 42–81 | 2007–2018 | BT/AT | NR | NR | Qualit./ Quant. | BMB/Follow-up | 0 | 3 | 1 | 35 |
| Xiao Xue et al., 2020 [29] | China | 55 | NR | NR | Adult. NR | 2016–2017 | BT | 2 weeks | Unilateral | Qualit. | BMB | NR | NR | NR | NR |
| Yağci-Küpeli et al., 2019 [30] | Turkey | 36 | M 26 F 10 | 7 Median | Pediatr. 2–17 | 2014–2017 | BT | NR | NR | Qualit./ Quant. | NR | NR | NR | NR | NR |
| Chen et al., 2019 [31] | China | 46 | M 36 F 10 | 7 Median | Pediatr. 2–18 | 2010–2017 | BT | NR | Unilateral | Qualit. | BMB/Follow-up | NR | NR | NR | NR |
| Abe et al., 2019 [32] | Japan | 83 | M 51 F 32 | 73 Median | Adult 63.5–78 | 2006–2018 | BT | NR | Unilateral | Qualit./ Quant. | BMB/Follow-up | NR | NR | 70 | |
| Badr et al., 2018 [33] | Egypt | 27 | M 20 F 7 | 7 Median | Pediatr. 2–16 | 2010–2015 | BT | 2 weeks | NR | Qualit./ Quant. | NR | 0 | 9 | 4 | 14 |
| Özpolat et al., 2018 [34] | Turkey | 22 | M 10 F 12 | 55 Mean | Adult NR | NR | BT | NR | Unilateral | Qualit. | BMB | 2 | 5 | 5 | 10 |
| Chen et al., 2018 [35] | China | 93 | M 66 F 27 | 8 Median | Pediatr. 1–21 | 2010–2017 | BT | 2 weeks | Unilateral | Qualit. | BMB/Follow-up | 8 | 11 | 51 | 23 |
| Öner et al., 2017 [36] | Turkey | 108 | NR | 45.3 Mean | Adult & Pediatr. 3–85 | 2009–2013 | BT/AT | 10 days | Unilateral | Qualit. | BMB | NR | NR | NR | NR |
| Teagle et al., 2017 [37] | UK | 36 | DLBCL M 16 F 8 FL M 4 F 8 | DLBCL 58/ FL 59 Median | Adult DLBCL 20–79 FL 33–71 | 2008–2013 | BT | DLBCL (0–104) FL (1–19) days | Unilateral | Qualit. | BMB | DLBCL 4 FL 2 | DLBCL 7 FL 2 | DLBCL 7 FL 5 | DLBCL 6 FL 3 |
| Albano et al., 2017 [38] | Italy | 57 | M 31 F 26 | 54.2 Mean | Adult 21–86 | 2013–2015 | NR | 10 days | NR | Qualit. | BMB | 1 | 13 | 9 | 34 |
| Pham et al., 2017 [39] | USA | 16 | M 11 F 5 | 63 Median | Adult 34–72 | 2001–2015 | BT/AT | 30 days | NR | Qualit. | NR | NR | NR | NR | NR |
| El Karak et al., 2017 [40] | Lebanon | 54 | M 25 F 29 | 50 Mean | Adult 16–87 | 2009–2013 | BT | NR | NR | Qualit./ Quant. | BMB | 10 | 12 | 10 | 22 |
| Yilmaz et al., 2017 [41] | Turkey | 201 | M 113 F 88 | 59 Median | Adult 21–87 | 2007–2013 | NR | <7 days | Unilateral | Qualit./ Quant. | NR | NR | NR | NR | NR |
| Vishnu et al., 2017 [42] | USA | 99 | M 57 F 42 | 62 Median | Adult 24–88 | 2004–2013 | BT | <2 weeks | Unilateral | Qualit. | BMB | NR | NR | NR | NR |
| Alzahrani et al., 2016 [43] | Denmark | 530 | M 294 F 267 | 65 Median | Adult 16–90 | 2007–2013 | BT | NR | Unilateral | Qualit. | BMB | 197 | 333 | ||
| Chen-Liang et al., 2015 [44] | Spain | 232 | M 120 F 112 | 58 Median | Adult 18–85 | 2009–2014 | BT | 30 days | Unilateral | Qualit./ Quant. | NR | 23 | 34 | 69 | 106 |
| Kim et al., 2015 [45] | South Korea | 86 | NR | NR | Adult NR | 2004–2009 | NR | NR | Unilateral | Qualit./ Quant. | BMB | NR | NR | NR | NR |
| Lee et al., 2015 [46] | Hong Kong | 46 | M 23 F 23 | 59 Mean | Adult | 2007–2014 | BT | 4 ± 9 days | Bilateral | Qualit./ Quant. | BMB/Follow-up | NR | NR | NR | NR |
| Adams et al., 2015 [47] | Netherlands | 40 | M 24 F 16 | 66 Mean | Adult 28–88 | 2007–2013 | BT | 0–15 days | Unilateral | Qualit. | BMB | NR | NR | NR | NR |
| Çetin et al., 2015 [48] | Turkey | 100 | M 59 F 41 | NR | Adult 18–85 | 2008–2012 | NR | NR | Unilateral | Qualit. | BMB | 1 | 42 | 28 | 29 |
| Cortés-Romera ** et al., 2014 [49] | Spain | 84 | M 43 F 41 | 62.5 Median | Adult 19–78 | 2004–2010 | BT | 2 weeks | Unilateral | Qualit./ Quant. | BMB | 14 | 28 | 13 | 29 |
| Adams et al., 2014b [50] | Netherlands | 78 | M 42 F 36 | 69 Median | Adult 33–88 | 2007–2013 | BT/AT | 0–26 days | Unilateral | Qualit. | BMB | NR | NR | 60 | |
| Adams et al. 2014c [51] | Netherlands | 22 | M 10 F 12 | 63.2 Mean | Adult 43–86 | 2007–2013 | BT | <30 days | Unilateral | Qualit./ Quant. | BMB | NR | NR | NR | NR |
| Berthet et al., 2013 [52] | France | 133 | NR | 57 Mean | Adult 18–87 | 2006–2011 | BT | <60 days | Unilateral | Qualit. | BMB/Follow-up | NR | NR | NR | NR |
| Khan et al., 2013 [53] | UK | 130 | M 77 F 53 | 59 Median | Adult 22–87 | 2005–2012 | BT | 1 month | Unilateral | Qualit. | BMB/Follow-up | 30 | 29 | 26 | 45 |
| Pelosi ** et al., 2011 [54] | Italy | 207 | NR | NR | Adult NR | 2004–2009 | BT/AT | 2 weeks | Bilateral | Qualit. | NR | 1 | 10 | 14 | 10 |
| Mittal et al., 2011 [55] | India | 77 | NR | NR | Adult NR | 2009–2010 | NR | 7–10 days | Bilateral | Qualit./ Quant. | NR | NR | NR | NR | NR |
| Reference | Sensitivity | Specificity | PPV | NPV | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NHL Subtype | BMB | PET/CT | BMB | PET/CT | BMB | PET/CT | BMB | PET/CT | ||
| Aguado-Vázquez et al., 2021 [15] | DLBCL | n = 154 | NR | 63.20% | NR | 80.00% | NR | 30.80% | NR | 93.90% |
| FL | n = 47 | NR | 78.60% | NR | 78.80% | NR | 61.10% | NR | 89.70% | |
| NHL | n = 96 | NR | 73.30% | NR | 85.20% | NR | 47.80% | NR | 94.50% | |
| Kaddu-Mulindwa et al., 2021 [16] | NHL | n = 930 | 38.00% | 84.00% | 100% | 100% | 100% | 100% | 84.00% | 95.00% |
| Göçer et. al., 2021 [17] | FL | n = 46 | NR | 31.50% | NR | 85.10% | NR | 60.00% | NR | 63.80% |
| DLBCL | n = 127 | NR | 36.80% | NR | 96.30% | NR | 63.60% | NR | 89.60% | |
| NHL | n = 58 | NR | 52.90% | NR | 87.50% | NR | 85.70% | NR | 56.70% | |
| Maisarah et al., 2021 [18] | DLBCL | n = 21 | NR | 100% | NR | 77.80% | NR | 42.90% | NR | 100% |
| Lim et al., 2021 [19] | DLBCL | n = 512 | NR | 59.30% | NR | 93.60% | NR | 54.70% | NR | 94.60% |
| Nakajima et al., 2020 [20] | FL | n = 261 | NR | 57.00% | NR | 82.00% | NR | 59.00% | NR | 81.00% |
| St-Pierre et al., 2020 [21] | FL | n = 548 | NR | 60.00% | NR | 80.00% | NR | NR | NR | NR |
| Al-Sabbagh et al., 2020 [22] | Aggressive | n = 89 | 50.00% | 95.83% | 100% | 100% | 100% | 100% | 84.42% | 98.48% |
| Kandeel et al., 2020 [23] | DLBCL | n = 88 | 68.80% | 66.70% | 100% | 89.70% | 100% | 76.90% | 84.90% | 83.90% |
| Kupik et al., 2020 [24] | NHL | n = 89 | 81.60% | 69.00% | 100% | 100% | 100% | 100% | 89.00% | 80.00% |
| Elamir et al., 2020 [25] | NHL | n = 57 | 53.60% | 96.40% | 100% | 100% | 100% | 100% | 69.00% | 96.70% |
| DLBCL | n = 27 | 53.30% | 100% | 100% | 100% | 100% | 100% | 63.20% | 100% | |
| Büyükşimşek et al., 2020 [26] | NHL | n = 269 | 55.00% | 65.00% | NR | NR | NR | NR | 73.40% | 78.00% |
| DLBCL | n = 186 | 47.00% | 72.30% | NR | NR | NR | NR | 70.10% | 81.70% | |
| FL | n = 34 | 60.00% | 66.70% | NR | NR | NR | NR | 75.00% | 78.30% | |
| MCL | n = 24 | 85.70% | 42.90% | NR | NR | NR | NR | 83.30% | 55.60% | |
| BL | n = 12 | 66.70% | 33.30% | NR | NR | NR | NR | 88.90% | 80.00% | |
| PMBCL | n = 13 | 66.70% | 33.30% | NR | NR | NR | NR | 90.90% | 83.30% | |
| Tezol et al., 2020 [27] | NHL | n = 20 | NR | 50.00% | NR | 50.00% | NR | 60.00% | NR | 40.00% |
| Yang et al., 2020 [28] | MCL | n = 39 | NR | 77.78% | NR | 86.67% | NR | 87.50% | NR | 76.47% |
| Xiao Xue et al., 2011 [29] | DLBCL | n = 55 | NR | 77.80% | NR | 89.10% | NR | NR | NR | NR |
| Yağci-Küpeli et al., 2019 [30] | NHL | n = 36 | 58.30% | 75.00% | 95.80% | 100% | 100% | 100% | 82.10% | 88.90% |
| Chen et al., 2019 [31] | NHL | n = 46 | 39.00% | 100% | 100% | 100% | NR | NR | NR | NR |
| Abe et al., 2019 [32] | PTCL | n = 83 | 60.70% | 89.30% | 100% | 100% | 100% | 100% | 83.30% | 94.80% |
| Badr et al., 2018 [33] | NHL | n = 27 | 35.89% | 100% | 100% | 98.00% | 100% | 95.10% | 80.20% | 100% |
| Özpolat et al., 2018 [34] | NHL | n = 22 | NR | 75.00% | NR | 64.00% | NR | 57.00% | NR | 95.00% |
| Chen et al., 2018 [35] | NHL | n = 93 | 56.00% | 95.00% | 100% | 98.00% | 100% | 97.00% | 74.00% | 96.00% |
| Öner et al., 2017 [36] | NHL | n = 108 | NR | 24.32% | NR | 90.14% | NR | 56.25% | NR | 69.57% |
| Teagle et al., 2017 [37] | DLBCL | n = 24 | NR | 100% | NR | 100% | NR | 100% | NR | 100% |
| FL | n = 12 | NR | 0% | NR | 72.70% | NR | 0% | NR | 88.90% | |
| Albano et al., 2017 [38] | NHL | n = 57 | NR | 50.00% | NR | 84.40% | NR | 36.40% | NR | 90.50% |
| Pham et al., 2017 [39] | NHL | n = 16 | NR | 20.00% | NR | 66.70% | NR | NR | NR | NR |
| El Karak et al., 2017 [40] | DLBCL | n = 54 | NR | 80.00% | NR | 80.00% | NR | 33.00% | NR | 98.00% |
| Yilmaz et al., 2017 [41] | DLBCL | n = 201 | NR | 91.30% | NR | 94.30% | NR | 67.70% | NR | 98.80% |
| Vishnu et al., 2017 [42] | DLBCL | n = 99 | NR | 86.00% | NR | 86.00% | NR | 50.00% | NR | 98.00% |
| Alzahrani et al., 2016 [43] | NHL | n = 530 | NR | 60.00% | NR | 79.00% | NR | 36.00% | NR | 91.00% |
| DLBCL | n = 48 | NR | 77.00% | NR | 79.00% | NR | 29.00% | NR | 97.00% | |
| Chen-Liang et al., 2015 [44] | NHL | n = 232 | 77.60% | 52.70% | NR | NR | NR | NR | 90.20% | 81.70% |
| DLBCL | n = 155 | 62.50% | 65.60% | NR | NR | NR | NR | 91.10% | 91.70% | |
| BL | n = 9 | 66.70% | 83.30% | NR | NR | NR | NR | 60.00% | 75.00% | |
| FL | n = 41 | 93.70% | 50.00% | NR | NR | NR | NR | 96.10% | 75.80% | |
| MCL | n = 27 | 95.20% | 28.60% | NR | NR | NR | NR | 87.70% | 28.60% | |
| Kim et al., 2015 [45] | Indolent | n = 11 | NR | 0% | NR | 100% | NR | 0% | NR | 64.00% |
| Aggressive | n = 75 | NR | 61.00% | NR | 96.00% | NR | 85.00% | NR | 89.00% | |
| Lee et al., 2015 [46] | Indolent | n = 46 | 96.00% | 84.00% | 100% | 95.00% | 100% | 95.00% | 95.00% | 83.00% |
| Adams et al., 2015 [47] | DLBCL | n = 40 | NR | 14.30% | NR | 100% | NR | NR | NR | NR |
| Çetin et al., 2015 [48] | Aggressive | n = 100 | NR | 51.70% | NR | 83.00% | NR | 55.50% | NR | 80.80% |
| Cortés-Romera et al., 2014 [49] | DLBCL | n = 84 | NR | 94.00% | NR | 87.00% | NR | 63.00% | NR | 98.00% |
| Adams et al., 2014b [50] | DLBCL | n = 78 | NR | 68.80% | NR | NR | NR | NR | NR | NR |
| Adams et al. 2014c [51] | FL | n= 22 | NR | 85.70% | NR | 87.50% | NR | NR | NR | NR |
| Berthet et al., 2013 [52] | DLBCL | n = 133 | 24.20% | 93.90% | 100% | 99.00% | 100% | 96.90% | 80.00% | 98.00% |
| Khan et al., 2013 [53] | DLBCL | n = 130 | 40.00% | 94.00% | 100% | 100% | NR | NR | NR | NR |
| Pelosi et al., 2011 [54] | Aggressive | n = 207 | 67.80% | 64.40% | NR | NR | NR | NR | NR | NR |
| DLBCL | n = 120 | 40.00% | 84.00% | NR | NR | NR | NR | NR | NR | |
| MCL | n = 7 | 100% | 16.50% | NR | NR | NR | NR | NR | NR | |
| FL | n = 48 | 81.00% | 61.90% | NR | NR | NR | NR | NR | NR | |
| Mittal et al., 2011 [55] | NHL | n = 77 | 82.00% | 88.00% | NR | 95% | NR | 93.00% | 91.30% | 100% |
| Aggressive | n = 60 | 76.00% | 100% | NR | 94% | NR | 93.00% | 85.30% | 100% | |
| Indolent | n = 17 | 100% | 50.00% | NR | 100% | NR | 100% | 100% | 70.00% | |
| Reference | Risk of Bias | Applicability Concerns | |||||
|---|---|---|---|---|---|---|---|
| Patients Sample | Index Test | Reference Standard | Flow and Timing | Patients Sample | Index Test | Reference Standard | |
| Aguado-Vázquez et al., 2021 [15] | L | L | L | UN | L | L | L |
| Kaddu-Mulindwa et al., 2021 [16] | L | L | L | UN | L | L | L |
| Göçer et. al., 2021 [17] | L | L | L | L | L | L | L |
| Maisarah et al., 2021 [18] | L | L | L | UN | L | L | L |
| Lim et al., 2021 [19] | L | L | L | L | L | L | L |
| Nakajima et al., 2020 [20] | L | L | L | UN | L | L | L |
| St-Pierre et al., 2020 [21] | L | L | L | UN | L | L | L |
| Al-Sabbagh et al., 2020 [22] | L | L | L | L | L | L | L |
| Kandeel et al., 2020 [23] | L | L | L | L | L | L | L |
| Kupik et al., 2020 [24] | UN | L | L | UN | L | L | L |
| Elamir et al., 2020 [25] | UN | L | L | L | L | L | L |
| Büyükşimşek et al., 2020 [26] | UN | UN | UN | L | L | L | L |
| Tezol et al., 2020 [27] | UN | L | L | UN | L | L | L |
| Yang et al., 2020 [28] | UN | L | L | UN | L | L | L |
| Xiao Xue et al., 2020 [29] | UN | L | L | L | L | L | L |
| Yağci-Küpeli et al., 2019 [30] | UN | L | L | UN | L | L | L |
| Chen et al., 2019 [31] | L | L | UN | UN | L | L | L |
| Abe et al., 2019 [32] | L | L | L | UN | L | L | L |
| Badr et al., 2018 [33] | UN | L | L | L | L | L | L |
| Özpolat et al., 2018 [34] | UN | L | L | UN | L | L | L |
| Chen et al., 2018 [35] | L | L | L | L | L | L | L |
| Öner et al., 2017 [36] | UN | L | L | L | L | L | L |
| Teagle et al., 2017 [37] | UN | L | L | H | L | L | L |
| Albano et al., 2017 [38] | UN | L | L | L | L | L | L |
| Pham et al., 2017 [39] | UN | L | UN | H | L | L | L |
| El Karak et al., 2017 [40] | L | L | L | UN | L | L | L |
| Yilmaz et al., 2017 [41] | UN | L | L | L | L | L | L |
| Vishnu et al., 2017 [42] | L | L | L | L | L | L | L |
| Alzahrani et al., 2016 [43] | UN | L | L | UN | L | L | L |
| Chen-Liang et al., 2015 [44] | L | L | UN | H | L | L | L |
| Kim et al., 2015 [45] | UN | L | L | UN | L | L | L |
| Lee et al., 2015 [46] | L | L | L | L | L | L | L |
| Adams et al., 2015 [47] | L | L | L | L | L | L | L |
| Cetin et al., 2015 [48] | L | L | L | UN | L | L | L |
| Cortés-Romera et al., 2014 [49] | UN | L | L | L | L | L | L |
| Adams et al., 2014b [50] | UN | L | L | L | L | L | L |
| Adams et al., 2014c [51] | L | L | L | L | L | L | L |
| Berthet et al., 2013 [52] | L | L | L | H | L | L | L |
| Khan et al., 2013 [53] | UN | L | L | H | L | L | L |
| Pelosi et al., 2011 [54] | L | L | L | L | L | L | L |
| Mittal et al., 2011 [55] | UN | L | L | L | L | L | L |
| Sensitivity (Median) | Specificity (Median) | PPV (Median) | NPV (Median) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No. Studies | Disease | [18F]FDG PET/CT | BMB | [18F]FDG PET/CT | BMB | [18F]FDG PET/CT | BMB | [18F]FDG PET/CT | BMB |
| 20 | DLBCL | 77.40% | 47.00% | 91.65% | 100.00% | 63.60% | 100.00% | 97.00% | 80.00% |
| 9 | FL | 60.00% | 81.00% | 81.00% | NR | 59.50% | NR | 79.65% | 85.55% |
| 4 | MCL | 60.34% | 95.20% | 86.67% | NR | 87.50% | NR | 55.60% | 71.65% |
| 2 | BL | 58.30% | 66.70% | NR | NR | NR | NR | 77.50% | 73% |
| 1 | PMBCL | 33.30% | 66.70% | NR | NR | NR | NR | 83.30% | 90.90% |
| 1 | PTCL | 89.30% | 60.70% | 100% | 100% | 100% | 100% | 94.80% | 83.30% |
| 41 | NHL | 73.30% | 56.00% | 89.70% | 100.00% | 63.30% | 100.00% | 92.45% | 83.65% |
| 12 | Indolent | 58.50% | 93.70% | 85.10% | 100.00% | 60.00% | 100.00% | 78.30% | 95.55% |
| 24 | Aggresive | 77.00% | 57.90% | 93.80% | 100.00% | 63.60% | 100.00% | 97.00% | 84.42% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almaimani, J.; Tsoumpas, C.; Feltbower, R.; Polycarpou, I. FDG PET/CT versus Bone Marrow Biopsy for Diagnosis of Bone Marrow Involvement in Non-Hodgkin Lymphoma: A Systematic Review. Appl. Sci. 2022, 12, 540. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020540
Almaimani J, Tsoumpas C, Feltbower R, Polycarpou I. FDG PET/CT versus Bone Marrow Biopsy for Diagnosis of Bone Marrow Involvement in Non-Hodgkin Lymphoma: A Systematic Review. Applied Sciences. 2022; 12(2):540. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020540
Chicago/Turabian StyleAlmaimani, Jawaher, Charalampos Tsoumpas, Richard Feltbower, and Irene Polycarpou. 2022. "FDG PET/CT versus Bone Marrow Biopsy for Diagnosis of Bone Marrow Involvement in Non-Hodgkin Lymphoma: A Systematic Review" Applied Sciences 12, no. 2: 540. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020540