Multidrug-Resistant Bacterial Infections in Geriatric Hospitalized Patients before and after the COVID-19 Outbreak: Results from a Retrospective Observational Study in Two Geriatric Wards

Abstract
:1. Introduction
2. Results
2.1. Patients
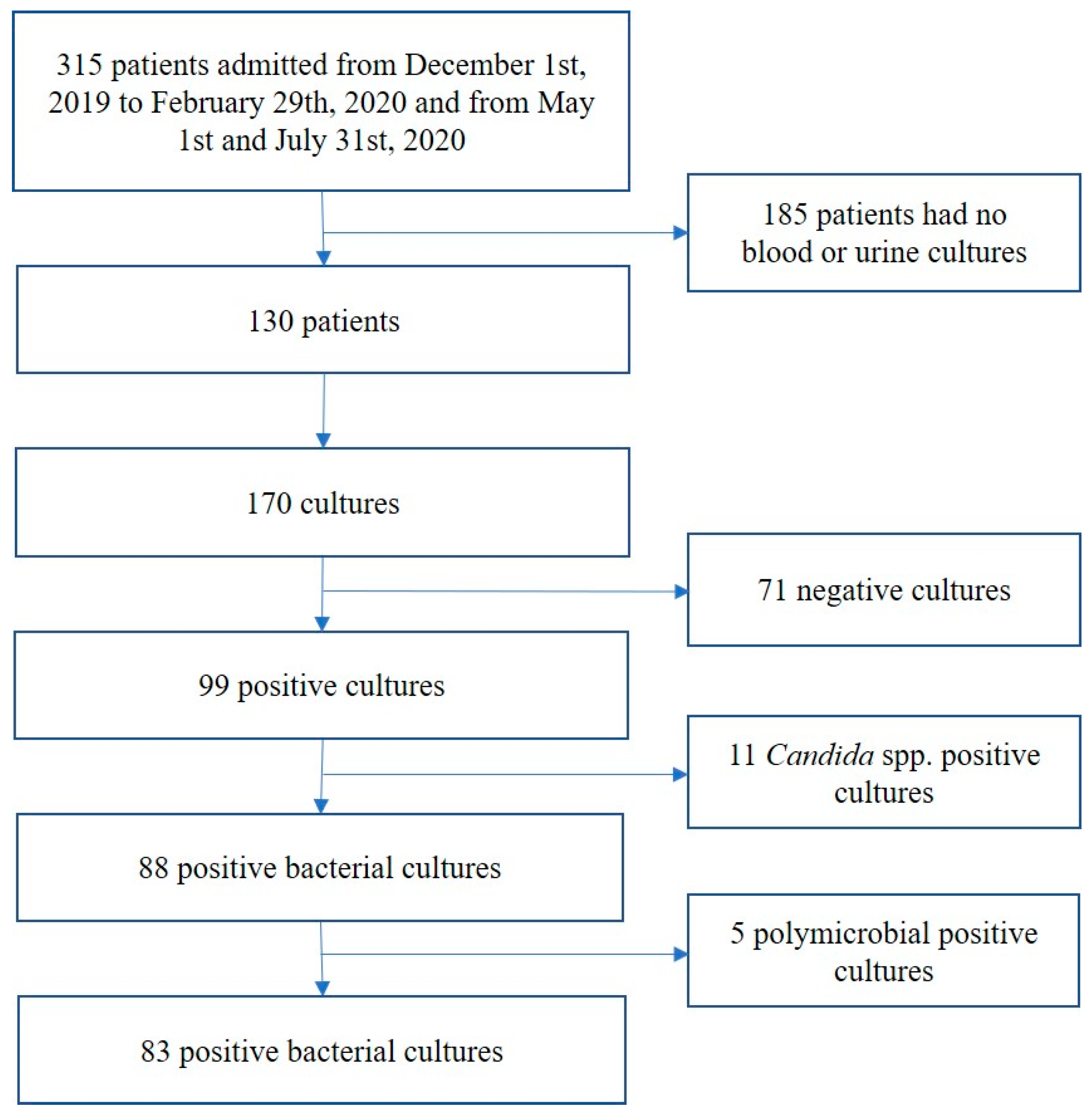
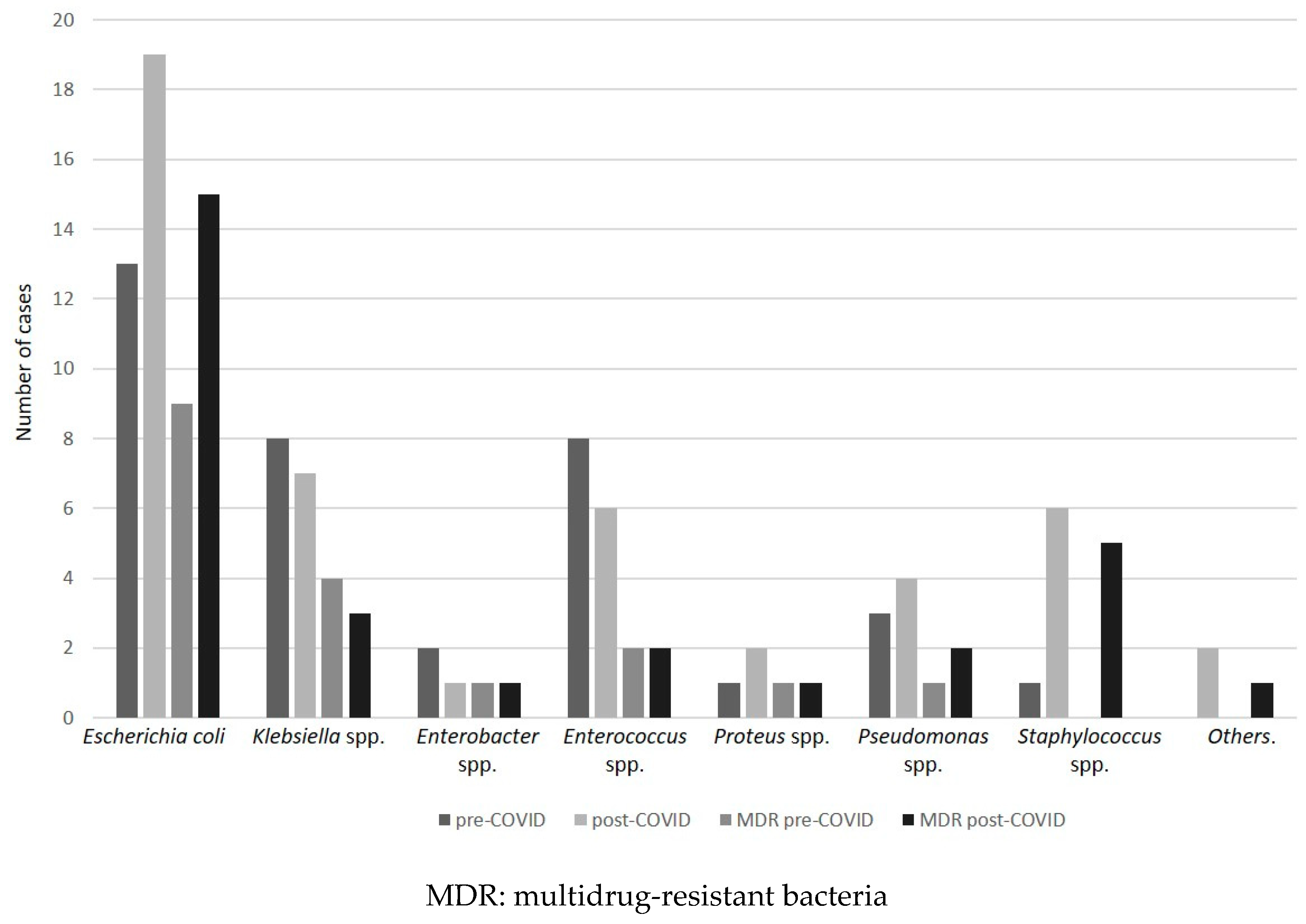
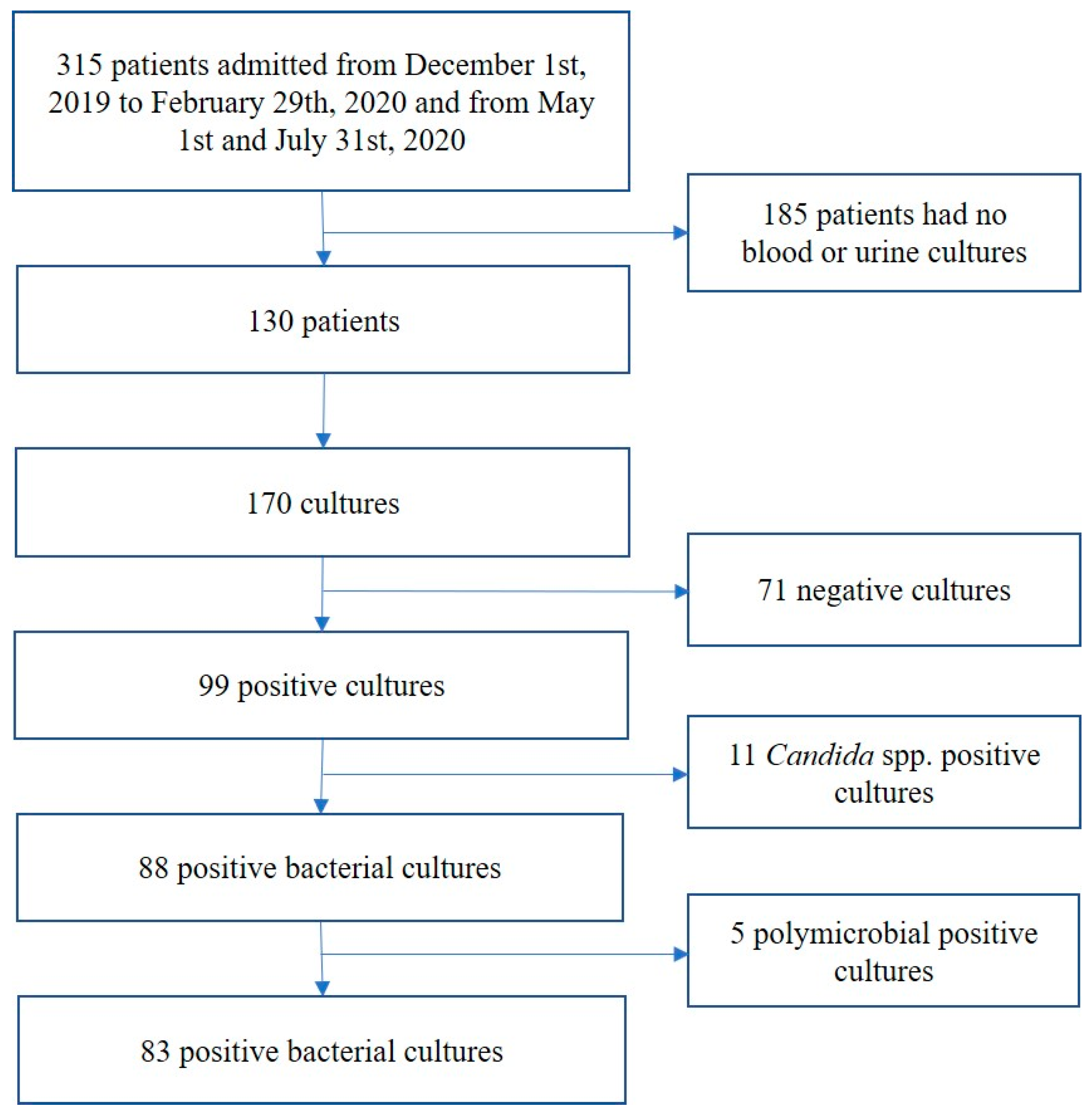
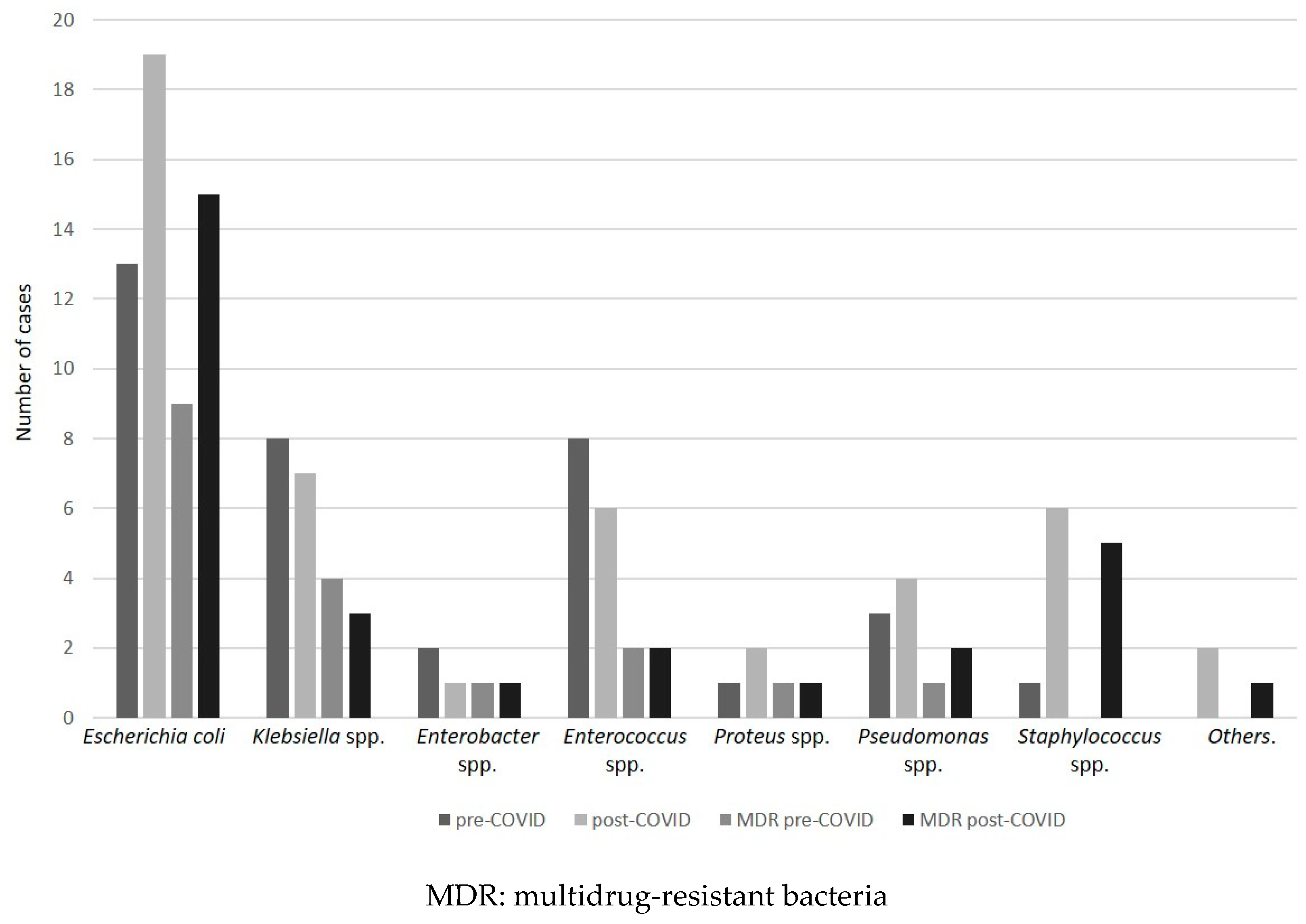
2.2. Cultures
2.3. Mortality
2.4. Antibiotics
3. Discussion
4. Materials and Methods
4.1. Inclusion and Exclusion Criteria
4.2. MDR
4.3. Patient Variables
4.4. Ethical Approval
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- No Time to Wait: Securing the Future from Drug-Resistant Infections Report to the Secretary-General of the United Nations April 2019. UN Interagency Coordination Group (IACG) on Antimicrobial Resistance. April 2019. Available online: https://www.who.int/antimicrobial-resistance/interagency-coordination-group/en/ (accessed on 28 December 2020).
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef] [PubMed]
- Council of Canadian Academies. When Antibiotics Fail; Council of Canadian Academies: Ottawa, ON, Canada, 2019; ISBN 978-1-926522-75-3. [Google Scholar]
- PHAC. Handle with Care: Preserving Antibiotics Now and Into the Future. In Chief Public Health Officer of Canada’s 2019 Spotlight Report; PHAC: Ottawa, ON, Canada, 2019. [Google Scholar]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal co-infection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 2, ciaa530. [Google Scholar] [CrossRef] [PubMed]
- Focà, E.; Rizzi, M.; Castelli, F.; Latronico, N.; Società Italiana di Malattie Infettive e Tropicali (SIMIT) Sezione Regione Lombardia; Gruppo Collaborativo-Terapia COVID-19. Vademecum per la cura delle Persone con Malattia da COVID-19 Versione 2.0. Available online: https://www.simit.org/news/11-vademecum-per-la-cura-delle-persone-con-malattia-da-covid-19 (accessed on 31 December 2020).
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Pandey, A.; Nikam, A.N.; Shreya, A.B.; Mutalik, S.P.; Gopalan, D.; Kulkarni, S.; Padya, B.S.; Fernandes, G.; Mutalik, S.; Prassl, R. Potential therapeutic targets for combating SARS-CoV-2: Drug repurposing, clinical trials and recent advancements. Life Sci. 2020, 256, 117883. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Smith, P.W.; Bennett, G.; Bradley, S.; Drinka, P.; Lautenbach, E.; Marx, J.; Mody, L.; Nicolle, L.; Stevenson, K. SHEA/APIC Guideline: Infection prevention and control in the long-term care facility. Am. J. Infect. Control 2008, 36, 504–535. [Google Scholar] [CrossRef] [Green Version]
- Detweiler, K.; Mayers, D.; Fletcher, S.G. Bacteruria and Urinary Tract Infections in the Elderly. Urol. Clin. N. Am. 2015, 42, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Mainous, A.G., 3rd; Diaz, V.A.; Matheson, E.M.; Gregorie, S.H.; Hueston, W.J. Trends in hospitalizations with antibiotic-resistant infections: U.S., 1997–2006. Public Health Rep. 2011, 126, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.Q.; Nguyen, N.T.Q.; Hughes, C.M.; O’Neill, C. Trends and impact of antimicrobial resistance on older inpatients with urinary tract infections (UTIs): A national retrospective observational study. PLoS ONE 2019, 14, e0223409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for Disease Control and Prevention (CDC). Information for Clinicians on Investigational Therapeutics for Patients with COVID-19. In Therapeutic Options for COVID-19 Patients|CDC; CDC: Atlanta, GA, USA, 2020. [Google Scholar]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.K. The Novel Coronavirus COVID-19 Outbreak: Global Implications for Antimicrobial Resistance. Front. Microbiol. 2020, 11, 1020. [Google Scholar] [CrossRef] [PubMed]
- Use of Antibiotics in an Influenza Pandemic. Scientific Evidence Base Review. Pandemic Influenza Preparedness Team, Department of Health, NHS. 2011. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/215669/dh_125424.pdf (accessed on 31 December 2020).
- Hsiao, C.Y.; Chen, T.H.; Lee, Y.C.; Hsiao, M.C.; Hung, P.H.; Wang, M.C. Risk factors for uroseptic shock in hospitalized patients aged over 80 years with urinary tract infection. Ann. Transl. Med. 2020, 8, 477. [Google Scholar] [CrossRef] [PubMed]
- Folliero, V.; Caputo, P.; Della Rocca, M.T.; Chianese, A.; Galdiero, M.; Iovene, M.R.; Hay, C.; Franci, G.; Galdiero, M. Prevalence and Antimicrobial Susceptibility Patterns of Bacterial Pathogens in Urinary Tract Infections in University Hospital of Campania “Luigi Vanvitelli” between 2017 and 2018. Antibiotics 2020, 9, 215. [Google Scholar] [CrossRef] [PubMed]
- Iacchini, S.; D’Ancona, F.; Bizzotti, V.; Giannitelli, S.; Monaco, M.; Errico, G.; Bellino, S.; Pezzotti, P.; Pantosti, A.; Iannazzo, S. CPE: Sorveglianza Nazionale Delle Batteriemie da Enterobatteri Produttori di Carbapenemasi. Dati 2019; Rapporti ISS Sorveglianza RIS-2/2020; Istituto Superiore di Sanità: Roma, Italy, 2020. [Google Scholar]
- Reale, M.; Strazzulla, A.; Quirino, A.; Rizzo, C.; Marano, V.; Postorino, M.C.; Mazzitelli, M.; Greco, G.; Pisani, V.; Costa, C.; et al. Patterns of multi-drug resistant bacteria at first culture from patients admitted to a third level University hospital in Calabria from 2011 to 2014: Implications for empirical therapy and infection control. Infez. Med. 2017, 25, 98–107. [Google Scholar] [PubMed]
- Vincitorio, D.; Barbadoro, P.; Pennacchietti, L.; Pellegrini, I.; David, S.; Ponzio, E.; Prospero, E. Risk factors for catheter-associated urinary tract infection in Italian elderly. Am. J. Infect. Control 2014, 42, 898–901. [Google Scholar] [CrossRef] [PubMed]
- Naylor, N.R.; Atun, R.; Zhu, N.; Kulasabanathan, K.; Silva, S.; Chatterjee, A.; Knight, G.M.; Robotham, J.V. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrob. Resist. Infect. Control 2018, 7, 58. [Google Scholar] [CrossRef] [PubMed]
- Bonazzetti, C.; Morena, V.; Giacomelli, A.; Oreni, L.; Casalini, G.; Galimberti, L.R.; Bolis, M.; Rimoldi, M.; Ballone, E.; Colombo, R.; et al. Unexpectedly High Frequency of Enterococcal Bloodstream Infections in Coronavirus Disease 2019 Patients Admitted to an Italian ICU: An Observational Study. Crit. Care Med. 2021, 49, e31–e40. [Google Scholar] [CrossRef] [PubMed]
- Bogossian, E.G.; Taccone, F.S.; Izzi, A.; Yin, N.; Garufi, A.; Hublet, S.; Njimi, H.; Ego, A.; Gorham, J.; Byl, B.; et al. The Acquisition of Multidrug-Resistant Bacteria in Patients Admitted to COVID-19 Intensive Care Units: A Monocentric Retrospective Case Control Study. Microorganisms 2020, 8, 1821. [Google Scholar] [CrossRef] [PubMed]
- Guisado-Gil, A.B.; Infante-Domínguez, C.; Peñalva, G.; Praena, J.; Roca, C.; Navarro-Amuedo, M.D.; Aguilar-Guisado, M.; Espinosa-Aguilera, N.; Poyato-Borrego, M.; Romero-Rodríguez, N.; et al. Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections. Antibiotics 2020, 9, 816. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 90. 2019. Available online: https://eucast.org/clinical_breakpoints/ (accessed on 12 December 2020).
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Total Sample N = 73 | Pre-COVID-19 N = 33 | Post-COVID-19 N = 40 | p | |
|---|---|---|---|---|
| Age (mean ± SD) | 87.4 ± 5.9 | 88.8 ± 5.9 | 86.1 ± 5.7 | 0.054 |
| Male (N, %) | 20 (27.4) | 8 (24.2) | 12 (30.0) | 0.532 |
| Functional status (mean ± SD) | ||||
| ADL preserved | 1.2 ± 1.6 | 1.3 ± 1.5 | 1.1 ± 1.7 | 0.461 |
| IADL preserved | 0.4 ± 1.2 | 0.5 ± 1.3 | 0.3 ± 1.1 | 0.662 |
| Mobility (N, %) | 0.934 | |||
| Bedridden | 31 (42.5) | 14 (42.4) | 17 (42.5) | |
| Bed-chair | 19 (26.0) | 8 (24.2) | 11 (27.5) | |
| Walking aid | 20 (27.4) | 10 (30.3) | 10 (25.0) | |
| Autonomous | 3 (4.1) | 1 (3.0) | 2 (5.0) | |
| Drugs taken daily (mean ± SD) | 6.7 ± 2.8 | 6.3 ± 3.3 | 7.2 ± 2.3 | 0.220 |
| Chronic diseases (mean ± SD) | 6.1 ± 2.0 | 6.1 ± 2.2 | 6.1 ± 1.9 | 0.989 |
| Reason for admission | 0.188 | |||
| Infectious disease (N, %) | 37 (50.7) | 19 (57.6) | 18 (45.0) | |
| Other reasons (N, %) | 36 (49.3) | 14 (42.4) | 22 (55.0) | |
| Length of stay, days (mean ± SD) | 12.3 ± 7.0 | 11.4 ± 5.8 | 13.0 ± 7.9 | 0.318 |
| In-hospital mortality (N, %) | 24 (32.9) | 8 (24.2) | 16 (40.0) | 0.154 |
| among MDR infections | 14 (58.3) | 3 (37.5) | 11 (68.8) | 0.198 |
| 30-days mortality (N, %) | 30 (41.1) | 11 (33.3) | 19 (47.5) | 0.402 |
| among MDR infections | 18 (60.0) | 3(27.3) | 15 (78.9) | 0.012 |
| Total Positive Cultures N = 83 | Pre-COVID-19 N = 36 | Post-COVID-19 N = 47 | p | |
|---|---|---|---|---|
| Type of culture(N, %) | ||||
| Urinoculture | 62 (74.7) | 31 (86.1) | 31 (66.0) | 0.036 |
| Urinoculture with MDR | 33 (53.2) | 16 (51.6) | 17 (54.8) | 0.799 |
| Bloodstream culture | 21 (25.3) | 5 (13.9) | 16 (34.0) | 0.036 |
| Bloodstream with MDR | 13 (61.9) | 2 (40.0) | 11 (68.8) | 0.038 |
| MDR infections(N, %) | 46 (55.4) | 18 (50.0) | 28 (59.6) | 0.384 |
| MDR bacteria(N, %) | 0.956 | |||
| E. coli | 32 (38.6) | 13 (36.1) | 19 (40.4) | 0.689 |
| MDR | 24 (75) | 9 (69.2) | 15 (78.9) | 0.105 |
| Klebsiella spp. | 15 (18.1) | 8 (22.2) | 7 (14.9) | 0.390 |
| MDR | 7 (46.6) | 4 (50.0) | 3 (42.8) | 0.289 |
| Enterococcus spp. | 14 (16.9) | 8 (22.2) | 6 (12.8) | 0.254 |
| MDR | 4 (28.6) | 2 (25) | 2 (33.3) | 0.401 |
| Proteus spp. | 3 (3.6) | 1 (2.8) | 2 (4.2) | 0.721 |
| MDR | 2 (66.7) | 1 (100) | 1 (50) | 0.747 |
| Pseudomonas spp. | 7 (8.4) | 3 (8.3) | 4 (8.5) | 0.977 |
| MDR | 3 (42.8) | 1 (33.3) | 2 (50) | 0.831 |
| Others | 2 (2.4) | 0 (0) | 2 (4.2) | 0.210 |
| MDR | 0 (0) | 0 (0) | 0 (0) | - |
| Enterobacter spp. | 3 (3.6) | 2 (5.6) | 1 (2.1) | 0.407 |
| MDR | 1 (33.3) | 1 (50) | 0 (0) | 0.207 |
| Staphylococcus spp. | 7 (8.4) | 1 (2.8) | 6 (12.8) | 0.132 |
| MDR | 5 (71.4) | 0 (0) | 5 (83.3) | 0.058 |
| MRSA | 1 (1.2) | 0 (0) | 1 (2.1) | 0.482 |
| ESBL | 33 (39.8) | 15 (41.7) | 18 (38.3) | 0.705 |
| CPB | 9 (10.8) | 3 (8.3) | 6 (12.8) | 0.725 |
| Total Positive Cultures N = 83 | Pre-COVID-19 N = 36 | Post-COVID-19 N = 47 | p | |
|---|---|---|---|---|
| Amikacin | 6 (10.0) | 3 (10.7) | 3 (9.4) | 0.539 |
| Amoxicillin/clavulanic | 23 (46.9) | 11 (44.0) | 12 (50.0) | 0.674 |
| Ampicillin | 3 (27.3) | 1 (16.7) | 2 (40.0) | 0.387 |
| Ampicillin/sulbactam | 3 (27.3) | 1 (16.7) | 2 (40.0) | 0.387 |
| Cefepime | 16 (51.7) | 5 (71.4) | 11 (45.8) | 0.259 |
| Cefotaxime | 36 (63.2) | 17 (68) | 19 (59.4) | 0.503 |
| Ceftazidime | 32 (52.5) | 15 (53.6) | 17 (51.6) | 0.384 |
| Ciprofloxacin | 45 (64.3) | 24 (75) | 21 (55.3) | 0.860 |
| Clindamycin | 5 (71.4) | 1 (100) | 4 (66.7) | 0.495 |
| Erythromycin | 4 (57.1) | 1 (100) | 3 (50.0) | 0.999 |
| Ertapenem | 7 (12.3) | 3 (12) | 4 (12.5) | 0.954 |
| Fosfomycin | 12 (22.2) | 5 (20.8) | 7 (23.3) | 0.826 |
| Fusidic acid | 2 (28.6) | 0 (0) | 2 (33.3) | 0.999 |
| Gentamicin | 28 (35.9) | 12 (34.3) | 16 (37.2) | 0.789 |
| Imipenem | 3 (27.3) | 1 (16.7) | 2 (40.0) | 0.387 |
| Kanamycin | 13 (100) | 6 (100) | 7 (100) | - |
| Levofloxacin | 12 (80) | 4 (80) | 8 (80) | 0.999 |
| Linezolid | 1 (5.3) | 0 (0) | 1 (8.3) | 0.999 |
| Meropenem | 5 (8) | 2 (7.4) | 3 (8.5) | 0.179 |
| Nitrofurantoin | 1 (4.0) | 1 (8.3) | 0 (0) | 0.288 |
| Oxacillin | 7 (100) | 1 (100) | 6 (100) | - |
| Piperacillin/tazobactam | 16 (25.4) | 9 (32.1) | 7 (20.0) | 0.271 |
| Rifampicin | 2 (28.6) | 0 (0) | 2 (33.3) | 0.999 |
| Streptomycin | 9 (100) | 4 (100) | 5 (100) | - |
| Teicoplanin | 3 (16.7) | 1 (14.3) | 2 (18.2) | 0.999 |
| Tetracycline | 4 (57.1) | 1 (100) | 3 (50.0) | 0.233 |
| Tmt/sulfamethoxazole | 30 (46.9) | 15 (57.7) | 15 (39.5) | 0.118 |
| Tigecycline | 2 (3.9) | 1 (5.3) | 1 (3.1) | 0.704 |
| Vancomycin | 2 (12.5) | 1 (20) | 1 (9.1) | 0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasperini, B.; Cherubini, A.; Lucarelli, M.; Espinosa, E.; Prospero, E. Multidrug-Resistant Bacterial Infections in Geriatric Hospitalized Patients before and after the COVID-19 Outbreak: Results from a Retrospective Observational Study in Two Geriatric Wards. Antibiotics 2021, 10, 95. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010095
Gasperini B, Cherubini A, Lucarelli M, Espinosa E, Prospero E. Multidrug-Resistant Bacterial Infections in Geriatric Hospitalized Patients before and after the COVID-19 Outbreak: Results from a Retrospective Observational Study in Two Geriatric Wards. Antibiotics. 2021; 10(1):95. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010095
Chicago/Turabian StyleGasperini, Beatrice, Antonio Cherubini, Moira Lucarelli, Emma Espinosa, and Emilia Prospero. 2021. "Multidrug-Resistant Bacterial Infections in Geriatric Hospitalized Patients before and after the COVID-19 Outbreak: Results from a Retrospective Observational Study in Two Geriatric Wards" Antibiotics 10, no. 1: 95. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010095