
Using a Machine Learning Algorithm to Predict the Likelihood of Presence of Dental Caries among Children Aged 2 to 7

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
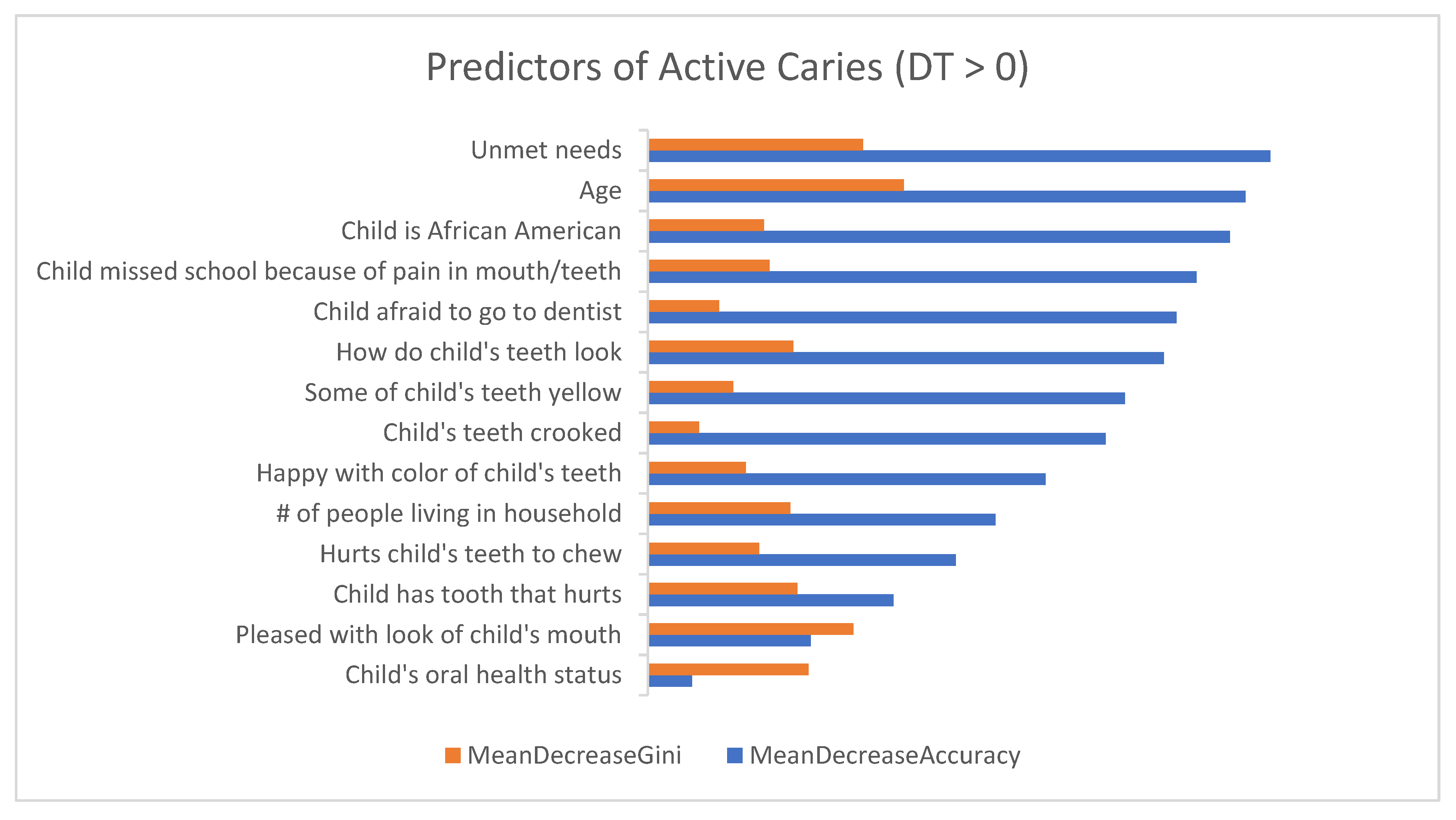
3.2. Questionnaire Items Predicting Active Caries
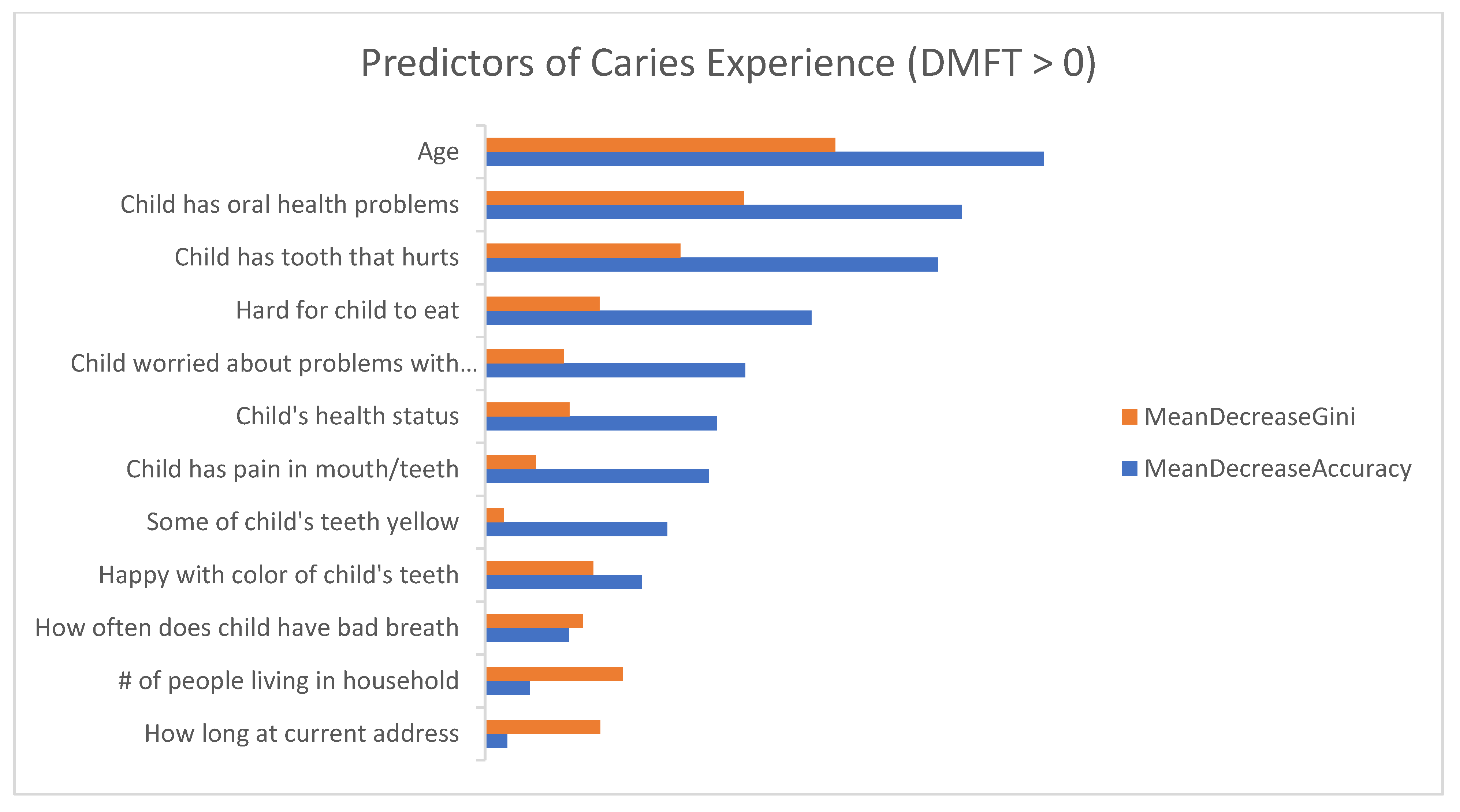
3.3. Questionnaire Items Predicting Caries Experience (Based on DMFT Index)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colak, H.; Dulgergil, C.T.; Dalli, M.; Hamidi, M.M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29–38. [Google Scholar]
- Anil, S.; Anand, P.S. Early childhood caries: Prevalence, risk factors, and prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef] [Green Version]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Elkstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeft, K.S.; Barker, J.C.; Shiboski, S.; Pantoja-Guzman, E.; Hiatt, R.A. Effectiveness evaluation of Contra Caries Oral Health Education Program for improving Spanish-speaking parents’ preventive oral health knowledge and behaviors for their young children. Community Dent. Oral Epidemiol. 2016, 44, 564–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Dental caries: Key Facts. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 13 November 2021).
- Peres, M.A.; Macpherson, L.; Weyent, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreno, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Hoeft, K. Using community participation to assess acceptability of “Contra Caries”, a theory- based, promotora-led oral health education program for rural Latino parents: A mixed methods study. BMC Oral Health 2015, 15, 103–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Disparities in Oral Health. 2021. Available online: https://www.cdc.gov/oralhealth/oral_health_disparities/index.htm (accessed on 13 November 2021).
- Fleming, E.; Afful, J. Prevalence of Total and Untreated Dental Caries among Youth: United States, 2015–2016. Available online: https://www.cdc.gov/nchs/data/databriefs/db307.pdf (accessed on 13 November 2021).
- Naavaal, S.; Kelekar, U. School hours lost due to acute/unplanned dental care. Health Behav. Policy Rev. 2018, 5, 66–73. [Google Scholar] [CrossRef]
- Barker, J.C.; Horton, S.B. An ethnographic study of Latino preschool children’s oral health in rural California: Intersections among family, community, provider and regulatory sectors. BMC Oral Health 2008, 31, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quock, R.L. The Evidence Supporting Fluoride Varnish. 2017. Available online: https://decisionsindentistry.com/article/evidence-supporting-fluoride-varnish/ (accessed on 13 November 2021).
- Bhanushali, P.; Katge, F.; Deshpande, S.; Chimata, V.K.; Shetty, S.; Pradhan, D. COVID-19: Changing trends and its impact on future of dentistry. Int. J. Dent. 2020, 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Marcus, M.; Wang, Y.; Xiong, D. Child and parent demographic characteristics and oral health perceptions associated with clinically measured oral health. JDR Clin. Transl. Res. 2018, 3, 302–313. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Hays, R.D.; Marcus, M.; Coulter, I.; Maida, C.; Ramos-Gomez, F.; Shen, J.; Wang, Y.; Spolsky, V.; Lee, S.; et al. Patient-reported oral health outcome measurement for children and adolescents. BMC Oral Health 2016, 16, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Hays, R.D.; Marcus, M.; Maida, C.A.; Shen, J.; Xiong, D.; Coulter, I.D.; Lee, S.Y.; Spolsky, V.W.; Crall, J.J.; et al. Developing children’s oral health assessment tool kits using machine learning algorithm. JDR Clin. Transl. Res. 2019, 11, 233–243. [Google Scholar]
- Maida, C.A.; Marcus, M.; Hays, R.D.; Coulter, I.D.; Ramos-Gomez, F.; Lee, S.Y.; McClory, P.S.; Van, L.V.; Wang, Y.; Shen, J.; et al. Child and adolescent perceptions of oral health over the life course. Qual. Life Res. 2015, 24, 2739–2751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maida, C.A.; Marcus, M.; Hays, R.D.; Coulter, I.D.; Ramos-Gomez, F.; Lee, S.Y.; McClory, P.S.; Van, L.V.; Wang, Y.; Shen, J.; et al. Qualitative methods in the development of a parent survey of children’s oral health status. J. Patient-Rep. Outcomes 2018, 2, 7. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.R.; Irwin, D.E.; Meier, A.; Varni, J.W.; DeWalt, D.A. The use of focus groups in the development of the PROMIS pediatrics item bank. Qual. Life Res. 2008, 17, 725–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL (TM): Measurement model for the pediatric quality of life inventory. Med. Care 1999, 37, 126. [Google Scholar] [CrossRef]
- Matza, L.S.; Patrick, D.L.; Riley, A.W.; Alexander, J.J.; Rajmil, L.; Pleil, A.M.; Bullinger, M. Pediatric patient-reported outcome instruments for research to support medical product labeling: Report of the ISPOR PRO good research practices for the assessment of children and adolescents task force. Value Health 2013, 16, 461–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, D.E.; Varni, J.W.; Yeatts, K.; DeWalt, D.A. Cognitive interviewing methodology in the development of a pediatric item bank: A patient reported outcomes measurement information system (PROMIS) study. Health Qual. Life Outcomes 2009, 7, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, A.L.; Gershen, J.A.; Marcus, M. Children’s oral health status index based on dentists’ judgment. JADA 1985, 110, 36–42. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Van denbroucke, J.P.; Strobe Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Eipdemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- STROBE: Strengthening the Reporting of Observational Studies in Epidemiology. Available online: https://www.strobe-statement.org/ (accessed on 14 November 2021).
- Marcus, M.; Xiong, D.; Wang, Y.; Maida, C.A.; Hays, R.D.; Coulter, I.D.; Spolsky, V.W.; Lee, S.Y.; Shen, J.; Crall, J.J.; et al. Development of toolkits for detecting dental caries and caries experience among children using self-report and parent report. Community Dent. Oral Epidemiol. 2019, 47, 520–527. [Google Scholar] [CrossRef]
- Cicchetti, D.V.; Feinstein, A.R. High agreement but low kappa: II. Resolving the paradoxes. J. Clin. Epidemiol. 1990, 43, 551–585. [Google Scholar] [CrossRef]
- Calle, M.L.; Urrea, V. Letter to the editor: Stability of random forest importance measures. Brief. Bioinform. 2011, 12, 86–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelleher, J.D.; Mac Namee, B.; D’arcy, A. Fundamentals of Machine Learning for Predictive Data Analytics: Algorithms, Worked Examples, and CAE Studies; MIT Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Yap, B.W.; Rani, K.A.; Rahman, H.A.A.; Fong, S.; Khairudin, Z.; Abdullah, N. An application of oversampling, undersampling, bagging and boosting in handling imbalanced datasets. In Proceedings of the First International Conference on Advanced Data and Information Engineering; Springer: Singapore, 2014; pp. 13–22. [Google Scholar]
- Pitts, N.B.; Baez, R.J.; Diaz-Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Seow, W.K.; Sharkov, N.; Songpaisan, Y.; et al. Early Childhood Caries: IAPD Bangkok Declaration. J. Dent. Child. 2019, 86, 72. [Google Scholar]
- Hurlbutt, M. CAMBRA: Best Practices in Dental Caries Management. 2011. Available online: https://pdfs.semanticscholar.org/f6ac/6833549fe10821f8baa6bb927e19bcfa8591.pdf (accessed on 21 October 2021).
- Wang, Y.; Hays, R.; Marcus, M.; Maida, C.; Shen, J.; Xiong, D.; Lee, S.; Spolsky, V.; Coulter, I.; Crall, J.; et al. Development of a parent’s short form survey of their children’s oral health. Int. J. Paediatr. Dent. 2019, 29, 332–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| 3-Fold Cross-Validation | Test | |||||||
|---|---|---|---|---|---|---|---|---|
| Tuning Parameter * | Threshold | Accuracy | Sensitivity | Specificity | Accuracy | Sensitivity | Specificity | |
| Active Caries | mtry = 41; ntree = 100 | 0.08 | 0.71 | 0.94 | 0.68 | 0.62 | 0.57 | 0.63 |
| Caries Experience | mtry = 2; ntree = 100 | 0.36 | 0.71 | 0.78 | 0.64 | 0.73 | 0.92 | 0.55 |
| Sample Characteristics | n (%) |
|---|---|
| Main Outcome Variables | |
| Active Caries | |
| Yes | 23 (13) |
| No | 159 (87) |
| Caries Experience (DMFT) | |
| Yes | 86 (47) |
| No | 96 (53) |
| Parent Demographics | |
| Age, years | |
| <30 | 42 (23) |
| 30–44 | 115 (63) |
| ≥45 | 25 (14) |
| Gender | |
| Male | 56 (31) |
| Female | 126 (69) |
| Race/ethnicity | |
| Caucasian/White | 45 (24) |
| African American | 14 (8) |
| Hispanic/Latino | 71 (39) |
| Asian | 21 (11) |
| Other | 31 (18) |
| Number of people in household | |
| ≤3 | 31 (17) |
| 4–5 | 101 (56) |
| ≥6 | 50 (27) |
| Number of years lived at current address | |
| ≤1 year | 33 (18) |
| >1 year–≤5 years | 82 (45) |
| >5 years–≤10 years | 36 (20) |
| >10 years | 31 (17) |
| Child’s Demographics | |
| Age, years | |
| 2 | 21 (12) |
| 3 | 25 (14) |
| 4 | 30 (16) |
| 5 | 22 (12) |
| 6 | 44 (24) |
| 7 | 40 (22) |
| Gender | |
| Male | 93 (51) |
| Female | 89 (49) |
| Race/ethnicity | |
| Caucasian/White | 43 (24) |
| African American | 14 (7) |
| Hispanic/Latino | 71 (39) |
| Asian | 21 (12) |
| Multi-racial | 21 (12) |
| Other | 12 (6) |
| Oral health-related predictor variables (survey questions) | |
| In general, would you say your child’s oral health status is: | |
| Excellent/very good | 120 (66) |
| Good | 50 (27) |
| Fair/poor | 12 (7) |
| During the last 12 months, did your child have an oral health problem? | |
| Yes | 55 (30) |
| No | 127 (70) |
| In the last 4 weeks, how much of the time were you pleased or happy with the look of your child’s mouth, teeth, jaws or gums? | |
| Always/almost always | 149 (82) |
| Often/sometimes | 30 (16) |
| Almost never/never | 3 (2) |
| In the last 4 weeks, how much of the time did your child have pain or discomfort with his/her mouth, tongue, teeth, jaws or gums? | |
| Always/almost always | 0 (0) |
| Often/sometimes | 14 (8) |
| Almost never/never | 168 (92) |
| How often does your child have bad breath? | |
| Always/almost always | 10 (6) |
| Often/sometimes | 91 (50) |
| Almost never/never | 81 (44) |
| When I look at my child’s teeth | |
| They look fine | 119 (66) |
| They could look a little better | 48 (26) |
| They could look a lot better | 15 (8) |
| In the last 4 weeks, how much of the time was your child worried or concerned about problems with his/her mouth, tongue, teeth, jaws or gums? | |
| Always/almost always | 1 (1) |
| Often/sometimes | 7 (4) |
| Almost never/never | 174 (95) |
| My child’s mouth hurts | |
| Always/almost always | 0 (0) |
| Often/sometimes | 9 (5) |
| Almost never/never | 173 (95) |
| My child has a tooth that hurts | |
| Always/almost always | 1 (1) |
| Often/sometimes | 15 (8) |
| Almost never/never | 166 (91) |
| It hurts my child’s teeth to chew | |
| Always/almost always | 0 (0) |
| Often/sometimes | 7 (4) |
| Almost never/never | 175 (96) |
| It is hard for my child to eat because of pain in his/her mouth | |
| Always/almost always | 0 (0) |
| Often/sometimes | 9 (5) |
| Almost never/never | 173 (95) |
| How happy are you with the color of your child’s teeth? | |
| Very much/quite a bit | 141 (78) |
| Somewhat | 24 (13) |
| A little bit/not at all | 17 (9) |
| Some of my child’s teeth are yellow | |
| Yes | 21 (12) |
| No | 161 (88) |
| My child’s teeth are crooked | |
| Yes | 15 (8) |
| No | 167 (92) |
| During the past 12 months, was there a time that your child needed dental care, but did not get it? | |
| Yes | 8 (4) |
| No | 174 (96) |
| How much is your child afraid to go to a dentist? | |
| Not at all | 97 (53) |
| A little bit/somewhat | 76 (42) |
| A great deal | 9 (5) |
| During the last school year, how many days of school did your child miss because of pain in his/her mouth, teeth, gums (if child goes to school)? | |
| Never | 168 (92) |
| 1 to 3 days | 13 (7) |
| 4 days or more | 1 (1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Gomez, F.; Marcus, M.; Maida, C.A.; Wang, Y.; Kinsler, J.J.; Xiong, D.; Lee, S.Y.; Hays, R.D.; Shen, J.; Crall, J.J.; et al. Using a Machine Learning Algorithm to Predict the Likelihood of Presence of Dental Caries among Children Aged 2 to 7. Dent. J. 2021, 9, 141. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9120141
Ramos-Gomez F, Marcus M, Maida CA, Wang Y, Kinsler JJ, Xiong D, Lee SY, Hays RD, Shen J, Crall JJ, et al. Using a Machine Learning Algorithm to Predict the Likelihood of Presence of Dental Caries among Children Aged 2 to 7. Dentistry Journal. 2021; 9(12):141. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9120141
Chicago/Turabian StyleRamos-Gomez, Francisco, Marvin Marcus, Carl A. Maida, Yan Wang, Janni J. Kinsler, Di Xiong, Steve Y. Lee, Ron D. Hays, Jie Shen, James J. Crall, and et al. 2021. "Using a Machine Learning Algorithm to Predict the Likelihood of Presence of Dental Caries among Children Aged 2 to 7" Dentistry Journal 9, no. 12: 141. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9120141