Clinical Failure and Emergence of Resistance during Third Generation Cephalosporin Therapy for Enterobacter spp. Infection: Is the Risk Overestimated? A Prospective Multicentric Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Characteristics of Patients
2.3. Clinical and Physiological Parameters
2.4. Definition
- -
- Impairment of lung function and infiltration in the chest X-ray film was observed;
- -
- Fever ≥ 38.3 °C or leukocytosis ≥ 10,000/µL was observed.
- -
- ≥104 CFU/mL from bronchoalveolar lavage (BAL) sample;
- -
- ≥103 CFU/mL from protected specimen brushing;
- -
- ≥105 CFU/mL from tracheal aspiration.
2.5. Microbiological Methods
2.6. Statistics
3. Results
3.1. Study Population
3.2. Characteristics of Population
3.3. Antibiotic Therapy
3.3.1. Third Generation Cephalosporin Therapy
3.3.2. First Antibiotic Therapy, Clinical Failure and Emergence of Resistance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Jacoby, G.A. AmpC beta-lactamases. Clin. Microbiol. Rev. 2009, 22, 161–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livermore, D.M.; Brown, D.F.; Quinn, J.P.; Carmeli, Y.; Paterson, D.L.; Yu, V.L. Should third-generation cephalosporins be avoided against AmpC-inducible Enterobacteriaceae? Clin. Microbiol. Infect. 2004, 10, 84–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, J.W.; Fine, M.J.; Shlaes, D.M.; Quinn, J.P.; Hooper, D.C.; Johnson, M.P.; Ramphal, R.; Wagener, M.M.; Miyashiro, D.K.; Yu, V.L. Enterobacter bacteremia: Clinical features and emergence of antibiotic resistance during therapy. Ann. Intern. Med. 1991, 115, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.S.; Cosgrove, S.; Harris, A.; Eliopoulos, G.M.; Carmeli, Y. Risk factors for emergence of resistance to broad-spectrum cephalosporins among Enterobacter spp. Antimicrob. Agents Chemother. 2001, 45, 2628–2630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.H.; Lee, J.E.; Park, S.J.; Choi, S.H.; Lee, S.O.; Jeong, J.Y.; Kim, M.N.; Woo, J.H.; Kim, Y.S. Emergence of antibiotic resistance during therapy for infections caused by Enterobacteriaceae producing AmpC beta-lactamase: Implications for antibiotic use. Antimicrob. Agents Chemother. 2008, 52, 995–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Antimicrobial susceptibility of Gram-negative organisms isolated from patients hospitalised with pneumonia in US and European hospitals: Results from the SENTRY Antimicrobial Surveillance Program, 2009–2012. Int. J. Antimicrob. Agents 2014, 43, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.N.; Ferguson, J.K. Antibiotic therapy for inducible AmpC β-lactamase-producing Gram-negative bacilli: What are the alternatives to carbapenems, quinolones and aminoglycosides? Int. J. Antimicrob. Agents 2012, 40, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Moy, S.; Sharma, R. Treatment Outcomes in Infections Caused by “SPICE” (Serratia, Pseudomonas, Indole-positive Proteus, Citrobacter, and Enterobacter) Organisms: Carbapenem versus Noncarbapenem Regimens. Clin. Ther. 2017, 39, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Bone, R.C.; Sprung, C.L.; Sibbald, W.J. Definitions for sepsis and organ failure. Crit. Care Med. 1992, 20, 724–726. [Google Scholar] [CrossRef] [PubMed]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- EUCAST: Clinical Breakpoints and Dosing of Antibiotics. Available online: http://www.eucast.org/clinical_breakpoints/ (accessed on 10 April 2021).
- Chaubey, V.P.; Pitout, J.D.; Dalton, B.; Gregson, D.B.; Ross, T.; Laupland, K.B. Clinical and microbiological characteristics of bloodstream infections due to AmpC β-lactamase producing Enterobacteriaceae: An active surveillance cohort in a large centralized Canadian region. BMC Infect. Dis. 2014, 14, 647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwaber, M.J.; Graham, C.S.; Sands, B.E.; Gold, H.S.; Carmeli, Y. Treatment with a broad-spectrum cephalosporin versus piperacillin-tazobactam and the risk for isolation of broad-spectrum cephalosporin-resistant Enterobacter species. Antimicrob. Agents Chemother. 2003, 47, 1882–1886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akova, M.; Yang, Y.; Livermore, D.M. Interactions of tazobactam and clavulanate with inducibly- and constitutively-expressed Class I beta-lactamases. J. Antimicrob. Chemother. 1990, 25, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, F.W. Cephalosporinase induction and cephalosporin resistance: A longstanding misinterpretation. Clin. Microbiol. Infect. 2002, 8, 823–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livermore, D.M. beta-Lactamases in laboratory and clinical resistance. Clin. Microbiol. Rev. 1995, 8, 557–584. [Google Scholar] [CrossRef] [PubMed]
- Pilmis, B.; Jullien, V.; Tabah, A.; Zahar, J.R.; Brun-Buisson, C. Piperacillin-tazobactam as alternative to carbapenems for ICU patients. Ann. Intensive Care 2017, 7, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulhunty, J.M.; Roberts, J.A.; Davis, J.S.; Webb, S.A.; Bellomo, R.; Gomersall, C.; Shirwadkar, C.; Eastwood, G.M.; Myburgh, J.; Paterson, D.L.; et al. Continuous infusion of beta-lactam antibiotics in severe sepsis: A multicenter double-blind, randomized controlled trial. Clin. Infect. Dis. 2013, 56, 236–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Füssle, R.; Biscoping, J.; Behr, R.; Sziegoleit, A. Development of resistance by Enterobacter cloacae during therapy of pulmonary infections in intensive care patients. Clin. Investig. 1994, 72, 1015–1019. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.I.; Kim, S.H.; Park, W.B.; Lee, K.D.; Kim, H.B.; Oh, M.D.; Kim, E.C.; Choe, K.W. Bloodstream infections caused by Enterobacter species: Predictors of 30-day mortality rate and impact of broad-spectrum cephalosporin resistance on outcome. Clin. Infect. Dis. 2004, 39, 812–818. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No. (%) of Patients | |
|---|---|
| Total | 74 (100) |
| Infection | |
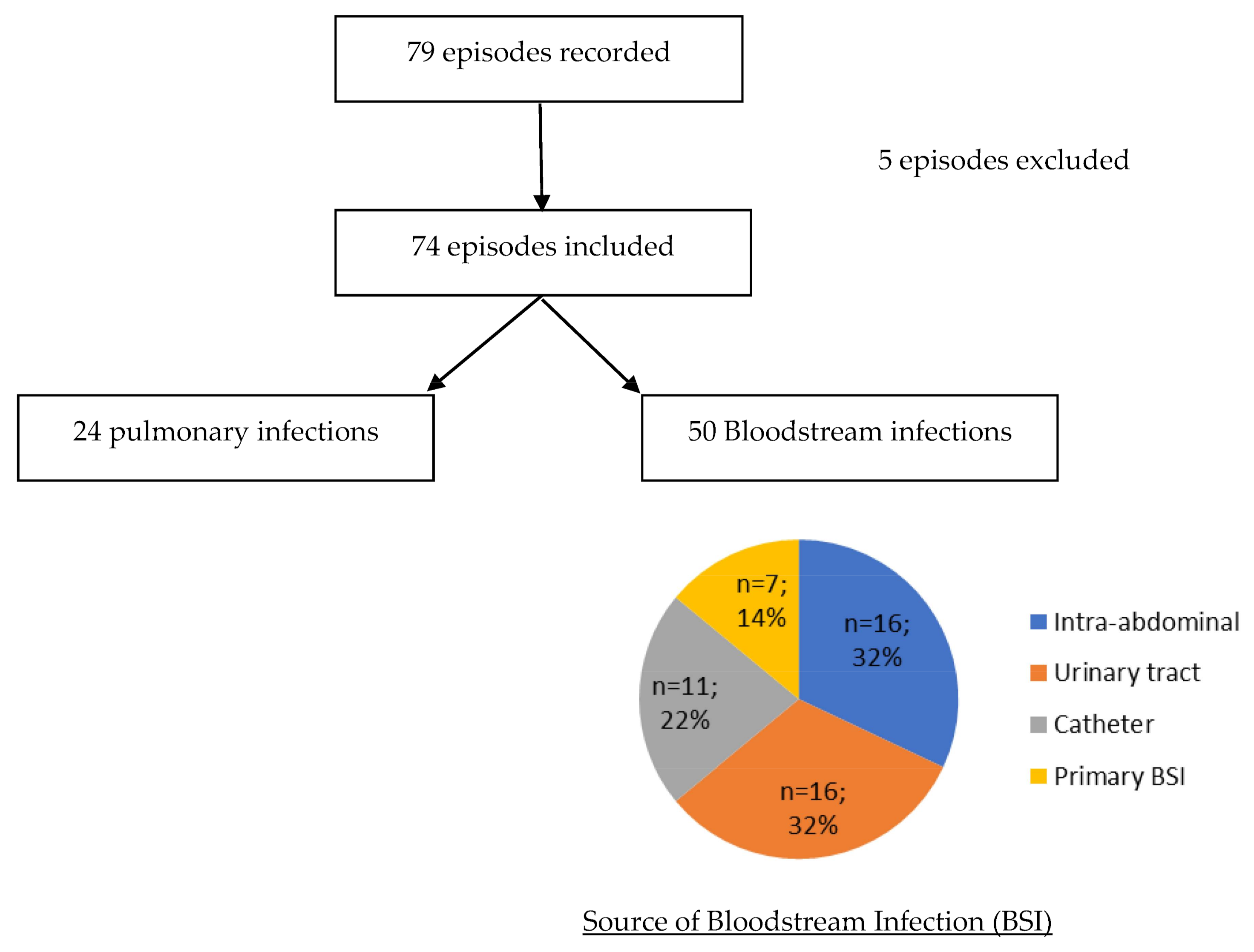
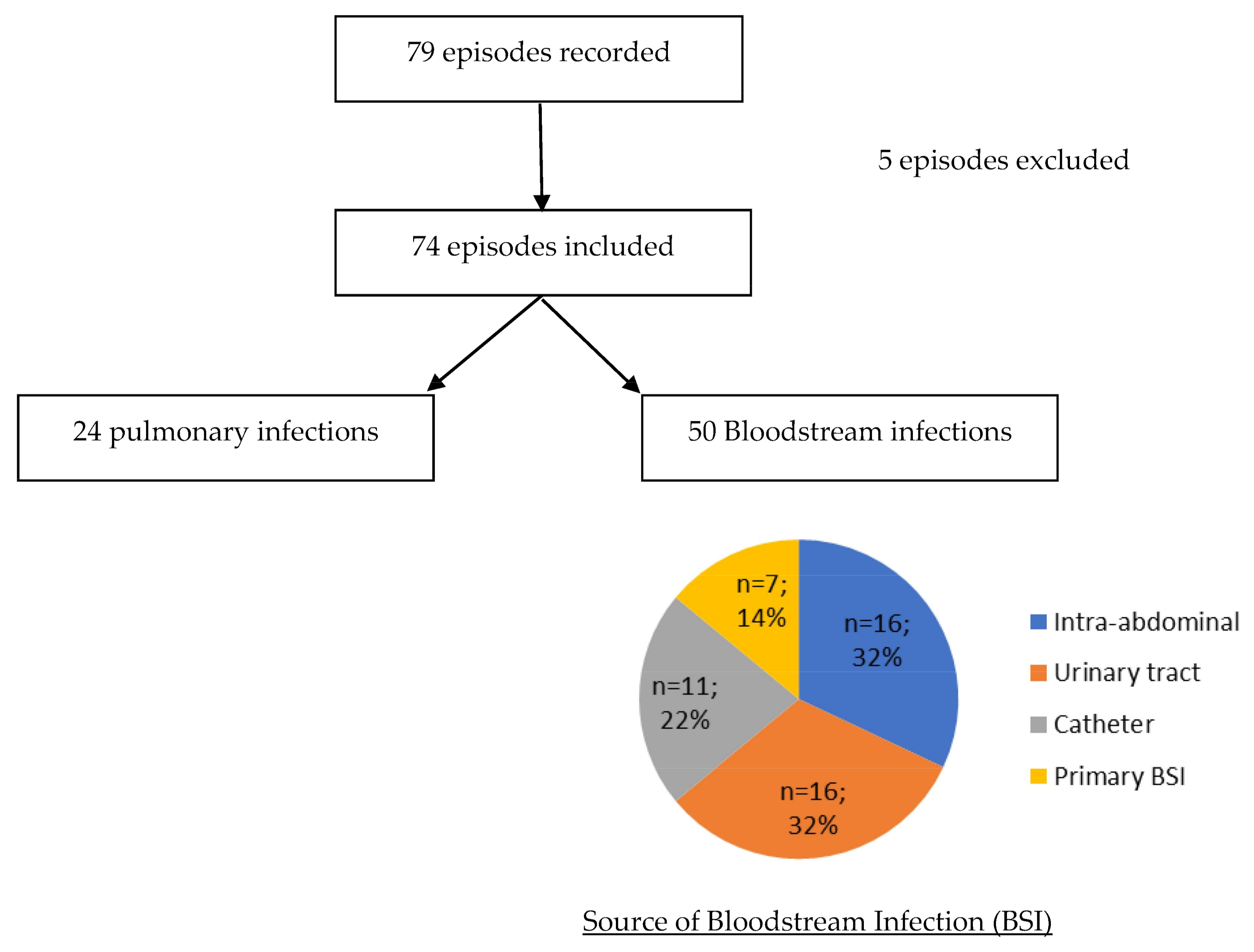
| BSI | 50 (67.6) |
| Respiratory tract infection without BSI | 24 (32.4) |
| Source of BSI | |
| Intra-abdominal | 16 (32) |
| Urinary tract | 16 (32) |
| Catheter | 11 (22) |
| Primary BSI | 7 (14) |
| Respiratory tract | 0 (0) |
| Male | 53 (71.6) |
| Age (median, [IQR]) | 69 [60.1–77.9] |
| Ward at the time of infection | |
| Medicine | 36 (48.6) |
| Intensive Care Unit | 31 (41.9) |
| Surgery | 6 (8.1 |
| Home | 1 (1.4) |
| Antibiotic therapy in the last 3 months | 39 (52.7) |
| Underlying disease | |
| Diabetes mellitus | 18 (24.3) |
| Chronic cardiac disease | 14 (18.9) |
| Chronic Respiratory disease | 14 (18.9) |
| Renal insufficiency | 10 (13.5) |
| Neutropenia (PNN < 500/mm3) | 0 (0) |
| Immunosuppressive treatment | 9 (12.2) |
| Corticosteroid use | 2 (2.7) |
| Hematologic malignancies | 2 (2.7) |
| Solid cancer | 32 (43.2) |
| Inflammatory disease | 0 (0) |
| HIV < 200 CD4/mm3 | 0 (0) |
| Charlson score (median, [IQR]) | 2 [1–4.75] |
| Severity of infection | |
| SOFA score (mean) | 5.9 ± 2.5 |
| Pitt score (mean) | 2.5 ± 1.2 |
| Biology (median, [IQR]) | |
| PCT (µg/L) | 2 [0.89–5.5] |
| CRP (mg/L) | 128 [71.3–223.5] |
| Leukocytes count (/mm3) | 12,600 [9330–19,300] |
| Creatininemia | 92 [56–165] |
| First-Line Treatment | Combination with Aminoglycoside | Combination with Fluoroquinolone | Treatment at 72 h | Definitive Treatment | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Duration (Days Mean) | No. (%) of Patients | Duration (Days Mean) | No. (%) of Patients | Duration (Days Mean) | No. of Patients | No. of Patients | |||||||||||||||
| 3GC | Fep | P ± TZ | Carb | FQ | SXT | AMC | Unknown | 3GC | Fep | P ± TZ | Carb | FQ | SXT | AMC | Unknown | ||||||
| Cefotaxime or ceftriaxone N = 26 | 5 | 2 (7.7) | 1 | 0 | 12 | 8 | 1 | 0 | 2 | 1 | 1 | 1 | 8 | 6 | 0 | 1 | 7 | 2 | 1 | 1 | |
| Cefepime N = 21 | 6.9 | 1 (4.8) | 2 | 1 (4.8) | 14 | 0 | 18 | 1 | 0 | 0 | 2 | 0 | 0 | 3 | 14 | 1 | 1 | 1 | 1 | 0 | 0 |
| Piperacillin± tazobactam N = 23 | 4.6 | 5 (21.8) | 1.8 | 2 (8.7) | 14 | 2 | 4 * | 15 | 1 | 0 | 0 | 0 | 1 | 3 | 4 | 11 | 1 | 1 | 1 | 0 | 2 |
| Carbapenem N = 4 | 12.5 | 2 (50) | 2 | 0 | 0 | 1 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 0 | 0 | |
| Total N = 74 | 5.8 | 10 (13.5) | 1.5 | 3 (4.1) | 14 | 14 (18.9) | 31 (41.9) | 17 (23.0) | 4 (5.4) | 2 (2.7) | 3 (4.1) | 1 (1.4) | 2 (2.7) | 14 (29.9) | 24 (32.4) | 12 (16.2) | 7 (9.5) | 9 (12.2) | 4 (5.4) | 1 (1.4) | 3 (4.1) |
| 3GC No. (%) | Non 3GC No. (%) | p Value | |
|---|---|---|---|
| Total | 26 (100) | 48 (100) | |
| Male | 22 (84.6) | 31 (64.6) | 0.10 |
| Age | 70 [57.8–76.3] | 67 [62.0–78.5] | 0.8 |
| Ward at the time of infection | |||
| Medicine | 17 (65.4) | 19 (39.6) | 0.5 |
| Surgery | 3 (11.5) | 3 (6.2) | 0.65 |
| ICU | 5 (19.2) | 26 (54.2) | <0.01 |
| Home | 1 (3.8) | 0 (0) | 0.35 |
| Antibiotic therapy in the last 3 months | 6(23.1) | 33 (69) | <0.01 |
| Underlying disease | |||
| Diabetes mellitus | 5 (19.2) | 13 (27.1) | 0.57 |
| Chronic cardiac disease | 9 (34.6) | 5 (10.4) | 0.02 |
| Chronic respiratory diseases | 2 (7.7) | 12 (25.0) | 0.11 |
| Renal insufficiency | 4 (15.4) | 6 (12.5) | 0.73 |
| Neutropenia | 0 | 0 | NA |
| Immunosuppressive treatment | 0 | 9 (18.8) | 0.02 |
| Corticosteroid use | 0 | 2(4.2) | 0.53 |
| Hematologic malignancies | 1 (42.3) | 1(2.1) | 1 |
| Solid cancer | 12 (46.1) | 20 (41.2) | 0.8 |
| Charlson score (median, [IQR]) | 2 [1–3] | 2 [1–5] | 1 |
| Pitt Score (median, [IQR]) | 2 [1–3.25] | 4 [2–6.25] | <0.01 |
| Site of infection | |||
| Respiratory tract | 3 (11.5) | 21 (43.8) | NA |
| Urinary tract | 10 (38.5) | 6 (12.5) | 0.02 |
| Catheter related | 4 (15.4) | 7 (14.6) | 0.53 |
| Intra-abdominal | 7 (26.9) | 9 (18.8) | 1 |
| Primary BSI | 2 (7.7) | 5 (10.4) | 0.8 |
| 3GC | Cefepime | Piperacillin ± Tazobactam | Carbapenem | |||||
|---|---|---|---|---|---|---|---|---|
| No. of Patients from Available Data (%) | p Value | No. of Patients from Available Data (%) | p Value | No. of Patients from Available Data (%) | p Value | No. of Patients from Available Data (%) | p Value | |
| Clinical improvement | 23/25 (92) | 0.53 | 20/20 (100) | 1.00 | 17/22 (77) | 0.08 | 2/3 (67) | 1.00 |
| Biological improvement | 13/21 (62) | 0.36 | 12/14 (86) | 0.30 | 11/17 (65) | 0.54 | 2/2 (100) | 1.00 |
| Emergence of 3GC resistance during treatment | 1/26 (4) | 1.00 | 0/21 (0) | 0.55 | 3/23 (13) | 0.08 | 0/0 (0) | 1.00 |
| 30-day Mortality | 1/26 (4) | 0.08 | 4/21 (19) | 0.45 | 5/23 (22) | 0.26 | 0/4 (0) | 1.00 |
| Patient | Sex | Age (Years) | Weight (Kg) | Ward | Charlson | Sofa Score | Creatinine Clearance (mL/min) | Source of Infection | Treatment 1 | Treatment 2 | Day of Emergence of Resistance (Site of Isolation) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotic | Dosage g/24h | Duration (Days) | Antibiotic | Dosage g/24 h | Duration (Days) | ||||||||||
| 1 | M | 31 | 41 | ICU | 8 | 2 | 64 | Pulmonary | 3GC | 3 | 2 | AMC | Un | 3 | 5 (pulmonary) |
| 2 | M | 64 | 109 | ICU | 2 | 7 | 136 | Pulmonary | Piperacillin tazobactam | 12 | 3 | No | NA | NA | 3 (pulmonary) |
| 3 | F | 21 | 56 | ICU | 1 | 7 | 155 | Catheter | Piperacillin tazobactam | 12 | 3 | No | NA | NA | 3 (bloodstream) |
| 4 | M | 83 | 95 | ICU | 4 | 5 | 16 | Pulmonary | Piperacillin tazobactam | NR | 4 | Cefotaxime | 3 | 3 | 7 (pulmonary) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilmis, B.; Delerue, T.; Belkacem, A.; Caraux-Paz, P.; Kernéis, S.; Alviset, S.; Canoui, E.; Mizrahi, A.; Bleibtreu, A.; Lafaurie, M.; et al. Clinical Failure and Emergence of Resistance during Third Generation Cephalosporin Therapy for Enterobacter spp. Infection: Is the Risk Overestimated? A Prospective Multicentric Study. Hygiene 2021, 1, 69-79. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene1020007
Pilmis B, Delerue T, Belkacem A, Caraux-Paz P, Kernéis S, Alviset S, Canoui E, Mizrahi A, Bleibtreu A, Lafaurie M, et al. Clinical Failure and Emergence of Resistance during Third Generation Cephalosporin Therapy for Enterobacter spp. Infection: Is the Risk Overestimated? A Prospective Multicentric Study. Hygiene. 2021; 1(2):69-79. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene1020007
Chicago/Turabian StylePilmis, Benoît, Thibaud Delerue, Anna Belkacem, Pauline Caraux-Paz, Solen Kernéis, Sophie Alviset, Etienne Canoui, Assaf Mizrahi, Alexandre Bleibtreu, Matthieu Lafaurie, and et al. 2021. "Clinical Failure and Emergence of Resistance during Third Generation Cephalosporin Therapy for Enterobacter spp. Infection: Is the Risk Overestimated? A Prospective Multicentric Study" Hygiene 1, no. 2: 69-79. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene1020007