Development, and Internal, and External Validation of a Scoring System to Predict 30-Day Mortality after Having a Traffic Accident Traveling by Private Car or Van: An Analysis of 164,790 Subjects and 79,664 Accidents

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Design and Participants
2.3. Ethical Aspects
2.4. Variables and Measurements
2.5. Sample Size
2.6. Statistical Methods
3. Results
4. Discussion
4.1. Summary
4.2. Strengths and Limitations
4.3. Comparison with the Existing Literature
4.4. Implications to Public Health and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Road Safety 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Wegman, F. The future of road safety: A worldwide perspective. IATSS Res. 2017, 40, 66–71. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Road Traffic Injuries. Available online: https://www.who.int/news-room/fact-sheets/detail/road-traffic-injuries (accessed on 1 September 2019).
- Goniewicz, K.; Goniewicz, M.; Pawłowski, W.; Fiedor, P. Road accident rates: Strategies and programmes for improving road traffic safety. Eur. J. Trauma Emerg. Surg. 2016, 42, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Thompson, J. On the road to prevention: Road injury and health promotion. Health Promot. J. Aust. 2014, 25, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Regidor, E.; Reoyo, A.; Calle, M.E.; Domínguez, V. Failure in the control of the number of traffic accident victims in Spain. Is this a result of the correct answer to the wrong question? Rev. Esp. Salud. Publica 2002, 76, 105–113. [Google Scholar] [CrossRef]
- Charters, K.E.; Gabbe, B.J.; Mitra, B. Population incidence of pedestrian traffic injury in high-income countries: A systematic review. Injury 2017, 48, 1331–1338. [Google Scholar] [CrossRef] [Green Version]
- Gómez-García, A.R.; Russo-Puga, M.; Suasnavas-Bermúdez, P.R.; Chérrez-Miño, M.C.; González-Jijón, L.A.; Celín-Ortega, F.A. Caracterización de la Mortalidad por Accidentes de Tránsito en Ecuador, 2015. Rev. Cienc. 2016, 5, 22–31. [Google Scholar]
- World Health Organization. World Report on Road Traffic Injury Prevention; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Odero, W.; Garner, P.; Zwi, A. Road traffic injuries in developing countries: A comprehensive review of epidemiological studies. Trop. Med. Int. Health 1997, 2, 445–460. [Google Scholar] [CrossRef]
- Moafian, G.; Aghabeigi, M.R.; Heydari, S.T.; Hoseinzadeh, A.; Lankarani, K.B.; Sarikhani, Y. An epidemiologic survey of road traffic accidents in Iran: Analysis of driver-related factors. Chin. J. Traumatol. 2013, 16, 140–144. [Google Scholar]
- La Torre, G.; Mannocci, A.; Quaranta, G.; La Torre, F. Determinants of traffic accident mortality in Italy, 1997–1999. Ital. J. Public Health 2006. [Google Scholar] [CrossRef]
- Olszewski, P.; Szagała, P.; Wolański, M.; Zielińska, A. Pedestrian fatality risk in accidents at unsignalized zebra crosswalks in Poland. Accid. Anal. Prev. 2015, 84, 83–91. [Google Scholar] [CrossRef]
- Sherafati, F.; Homaie-Rad, E.; Afkar, A.; Gholampoor-Sigaroodi, R.; Sirusbakht, S. Risk Factors of Road Traffic Accidents Associated Mortality in Northern Iran; A Single Center Experience Utilizing Oaxaca Blinder Decomposition. Bull. Emerg. Trauma 2017, 5, 116–121. [Google Scholar] [PubMed]
- Mehmandar, M.; Soori, H.; Amiri, M.; Norouzirad, R.; Khabzkhoob, M. Risk factors for fatal and nonfatal road crashes in Iran. Iran. Red. Crescent Med. J. 2014, 16, e10016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, G.; Ahmadi, B.; Pourreza, A.; Rahimi, A. Investigating prevalence of deaths from traffic accidents and factors associated with it in Yazd in 2009. J. Shahid. Sadoughi Univ. Med. Sci. 2014, 21, 831–839. [Google Scholar]
- Lankarani, K.B.; Heydari, S.T.; Aghabeigi, M.R.; Moafian, G.; Hoseinzadeh, A.; Vossoughi, M. The impact of environmental factors on traffic accidents in Iran. J. Inj. Violence Res. 2014, 6, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Jehle, D.; Gemme, S.; Jehle, C. Influence of obesity on mortality of drivers in severe motor vehicle crashes. Am. J. Emerg. Med. 2012, 30, 191–195. [Google Scholar] [CrossRef]
- Wong, J.-T.; Chung, Y.-S. Comparison of Methodology Approach to Identify Causal Factors of Accident Severity. Transp. Res. Rec. 2008, 2083, 190–198. [Google Scholar] [CrossRef]
- Quddus, M.A.; Wang, C.; Ison, S.G. Road Traffic Congestion and Crash Severity: Econometric Analysis Using Ordered Response Models. J. Traffic Transp. Eng. 2010, 136, 424–435. [Google Scholar] [CrossRef]
- Xie, Z.; Yan, J. Detecting traffic accident clusters with network kernel density estimation and local spatial statistics: An integrated approach. J. Transp. Geogr. 2013, 31, 64–71. [Google Scholar] [CrossRef]
- Michalaki, P.; Quddus, M.A.; Pitfield, D.; Huetson, A. Exploring the factors affecting motorway accident severity in England using the generalised ordered logistic regression model. J. Saf. Res. 2015, 55, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Dadashova, B.; Arenas Ramírez, B.; McWilliams, J.M.; Aparicio Izquierdo, F. The identification of patterns of interurban road accident frequency and severity using road geometry and traffic indicators. Transp. Res. Proc. 2016, 14, 4122–4129. [Google Scholar] [CrossRef] [Green Version]
- Santosa, S.P.; Mahyuddin, A.I.; Sunoto, F.G. Anatomy of Injury Severity and Fatality in Indonesian Traffic Accidents. J. Eng. Technol. Sci. 2017, 49, 412–422. [Google Scholar] [CrossRef] [Green Version]
- Halim, H. The pattern of severity of traffic accidents on traffic conditions heterogeneous. Int. J. Civ. Eng. Technol. 2017, 8, 1720–1729. [Google Scholar]
- Moons, K.G.; de Groot, J.A.; Bouwmeester, W.; Vergouwe, Y.; Mallett, S.; Altman, D.G.; Reitsma, J.B.; Collins, G.S. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: The CHARMS checklist. PLoS Med. 2014, 11, e1001744. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.M.; Wolff, R.F.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S. PROBAST: A Tool to Assess Risk of Bias and Applicability of Prediction Model Studies: Explanation and Elaboration. Ann. Intern. Med. 2019, 170, W1–W33. [Google Scholar] [PubMed] [Green Version]
- Wolff, R.F.; Moons, K.G.M.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; PROBAST Group. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Van Belleghem, G.; Devos, S.; De Wit, L.; Hubloue, I.; Lauwaert, D.; Pien, K.; Putman, K. Predicting in-hospital mortality of traffic victims: A comparison between AIS-and ICD-9-CM-related injury severity scales when only ICD-9-CM is reported. Injury 2016, 47, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Relaciones con las Cortes y de la Secretaría del Gobierno. Orden de 18 de Febrero de 1993 por la que se Modifica la Estadística de Accidentes de Circulación. Boletín Oficial del Estado, No. 47 (24-2-1993); Ministerio de Relaciones con las Cortes y de la Secretaría del Gobierno: Madrid, Spain, 1993. [Google Scholar]
- Ministerio de Relaciones con las Cortes y de la Secretaría del Gobierno. Orden INT/2223/2014, de 27 de Octubre, por la que se Regula la Comunicación de la Información al Registro Nacional de Víctimas de Accidentes de Tráfico. Boletín Oficial del Estado, No 289, (29-11-2014); Ministerio de Relaciones con las Cortes y de la Secretaría del Gobierno: Madrid, Spain, 2014. [Google Scholar]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Multivariate Imputation by Chained Equations. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar]
- Hastie, T.J. Generalized additive models. In Statistical Models in S; Chambers, J.M., Hastie, T.J., Eds.; Wadsworth & Brooks/Cole: Pacific Grove, CA, USA, 1992. [Google Scholar]
- Sullivan, L.M.; Massaro, J.M.; D’Agostino, R.B., Sr. Presentation of multivariate data for clinical use: The Framingham Study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.B.; Sullivan, L.M.; Levy, D.; Pencina, M.J.; Massaro, J.M.; D’Agostino, R.B., Sr.; Newton-Cheh, C.; Yamamoto, J.F.; Magnani, J.W.; Tadros, T.M.; et al. Development of a risk score for atrial fibrillation (Framingham Heart Study): A community-based cohort study. Lancet 2009, 373, 739–745. [Google Scholar] [CrossRef] [Green Version]
- Van Calster, B.; Nieboer, D.; Vergouwe, Y.; De Cock, B.; Pencina, M.J.; Steyerberg, E.W. A calibration hierarchy for risk models was defined: From utopia to empirical data. J. Clin. Epidemiol. 2016, 74, 167–176. [Google Scholar] [CrossRef]
- Azami-Aghdash, S.; Aghaei, M.H.; Sadeghi-Bazarghani, H. Epidemiology of Road Traffic Injuries among Elderly People, A Systematic Review and Meta-Analysis. Bull. Emerg. Trauma 2018, 6, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Azami-Aghdash, S.; Sadeghi-Bazarghani, H.; Heydari, M.; Rezapour, R.; Derakhshani, N. Effectiveness of Interventions for Prevention of Road Traffic Injuries in Iran and Some Methodological Issues: A Systematic Review. Bull. Emerg. Trauma 2018, 6, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Lefio, Á.; Bachelet, V.C.; Jiménez-Paneque, R.; Gomolán, P.; Rivas, K. A systematic review of the effectiveness of interventions to reduce motor vehicle crashes and their injuries among the general and working populations. Rev. Panam. Salud. Publica 2018, 42, e60. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Variable | Development Cohort n(%)/x ± s | Validation Cohort n(%)/x ± s |
|---|---|---|
| Accidents (Development n = 41,082; Validation n = 38,682) | ||
| Weekend: | ||
| Yes | 9567 (23.3) | 8965 (23.2) |
| No | 31,515 (76.7) | 29,717 (76.8) |
| Time (hours) 1 | 14.0 ± 5.2 | 14.0 ± 5.2 |
| Number of vehicles 1 | 1.9 ± 0.7 | 1.9 ± 0.7 |
| Road: | ||
| Urban | 26,649 (64.9) | 24,659 (63.7) |
| Interurban | 14,433 (35.1) | 14,023 (36.3) |
| Brightness: | ||
| Daylight | 29,531 (71.9) | 27,605 (71.4) |
| Dusk | 2267 (5.5) | 2195 (5.7) |
| Night (sufficient lighting) | 6728 (16.4) | 6334 (16.4) |
| Night (insufficient lighting) | 2556 (6.2) | 2548 (6.6) |
| Weather: | ||
| Good | 34,219 (83.3) | 31,818 (82.3) |
| Fog | 280 (0.7) | 292 (0.8) |
| Rain or hail | 3036 (7.4) | 2816 (7.3) |
| Snowing | 50 (0.1) | 54 (0.1) |
| High wind | 185 (0.5) | 130 (0.3) |
| Other | 1372 (3.3) | 1780 (4.6) |
| Missing | 1940 (4.7) | 1792 (4.6) |
| Vehicles (Development n = 59,807; Validation n = 56,302) | ||
| Type: | ||
| Private car | 54,502 (91.1) | 51,202 (90.9) |
| Van | 5305 (8.9) | 5100 (9.1) |
| Age of the vehicle (years): | ||
| x ± s | 10.3 ± 5.8 | 10.3 ± 5.9 |
| Missing | 16,580 (27.7) | 15,488 (27.5) |
| Other vehicles in the accident: | ||
| Private car | 31,573 (52.8) | 29,554 (52.5) |
| Van | 3821 (6.4) | 3732 (6.6) |
| Truck | 2243 (3.8) | 2179 (3.9) |
| Bicycle | 2042 (3.4) | 1971 (3.5) |
| Motorbike or moped | 10,899 (18.2) | 10,074 (17.9) |
| Heavy equipment or tractor | 129 (0.2) | 114 (0.2) |
| Bus | 561 (0.9) | 518 (0.9) |
| People (Development n = 84,502; Validation n = 80,288) | ||
| 30-day mortality: | ||
| Yes | 399 (0.5) | 379 (0.5) |
| No | 84,103 (99.5) | 79,909 (99.5) |
| Gender: | ||
| Male | 50,488 (59.7) | 47,898 (59.7) |
| Female | 32,717 (38.7) | 31,199 (38.9) |
| Missing | 1297 (1.5) | 1191 (1.5) |
| Age (years): | ||
| x ± s | 39.6 ± 17.1 | 39.4 ± 17.1 |
| Missing | 3294 (3.9) | 3130 (3.9) |
| Seat belt: | ||
| Yes | 61,687 (73.2) | 58,811 (73.3) |
| No | 1984 (2.3) | 2001 (2.5) |
| Missing | 20,651 (24.4) | 19,476 (24.3) |
| Position in the vehicle: | ||
| Driver | 59,731 (70.7) | 56,192 (70.0) |
| Front passenger | 14,274 (16.9) | 13,708 (17.1) |
| Rest of passengers | 10,497 (12.4) | 10,388 (12.9) |
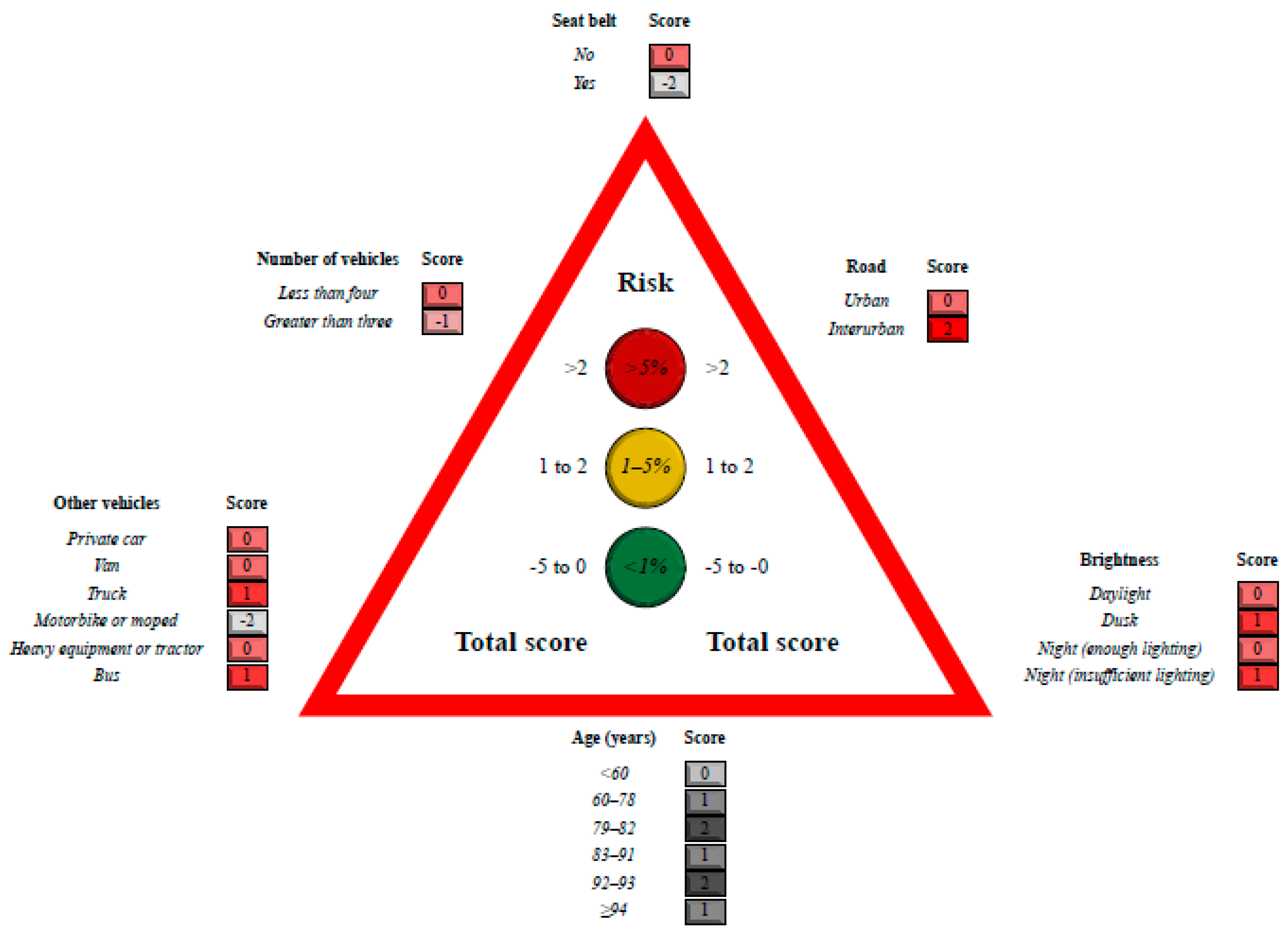
| Variable | B (SE) | p-Value |
|---|---|---|
| Number of vehicles | −0.27 (0.11) | 0.012 |
| Interurban road | 2.53 (0.20) | <0.001 |
| Brightness: | ||
| Dusk | 0.96 (0.19) | <0.001 |
| Night (insufficient lighting) | 1.03 (0.13) | <0.001 |
| Weather: | ||
| Rain or hail | −0.35 (0.20) | 0.075 |
| Gender male | 0.43 (0.12) | <0.001 |
| Other vehicles in the accident: | ||
| Private car | −0.43 (0.18) | 0.013 |
| Motorbike or moped | −2.67 (0.72) | <0.001 |
| Van | −0.48 (0.27) | 0.08 |
| Truck | 1.32 (0.18) | <0.001 |
| Bus | 1.00 (0.45) | 0.028 |
| Age (years): | ||
| S2 | 1.29 (0.56) | 0.022 |
| S3 | 1.16 (0.34) | 0.001 |
| S4 | 2.77 (0.54) | <0.001 |
| S5 | 3.92 (0.54) | <0.001 |
| S6 | 2.92 (1.43) | 0.042 |
| Time (hours): | ||
| S5 | −0.95 (0.28) | 0.001 |
| Seat belt | −2.54 (0.13) | <0.001 |
| Age of the vehicle (years): | ||
| S3 | 0.25 (0.18) | 0.168 |
| Intercept | −6.26 (0.43) | <0.001 |
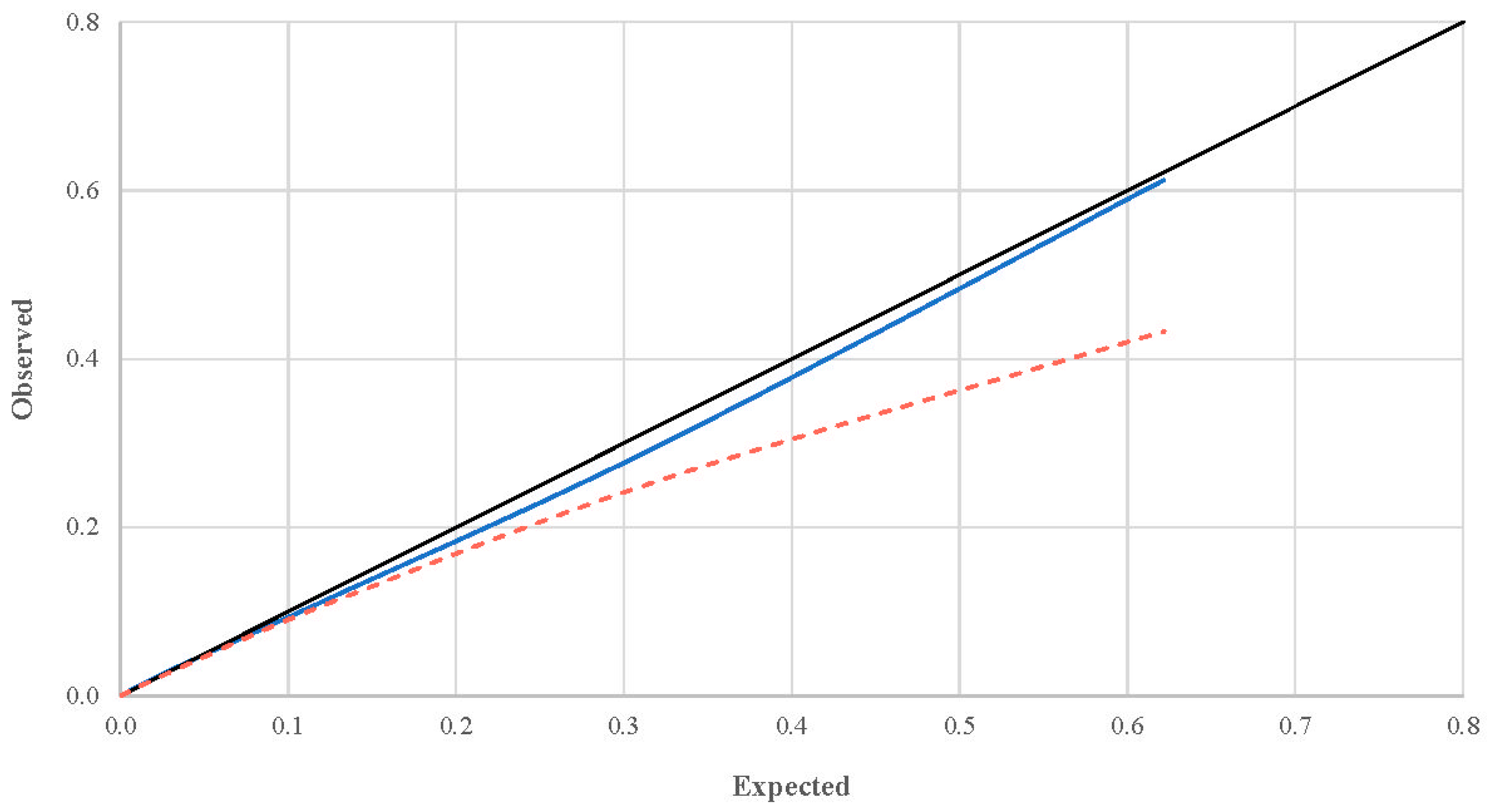
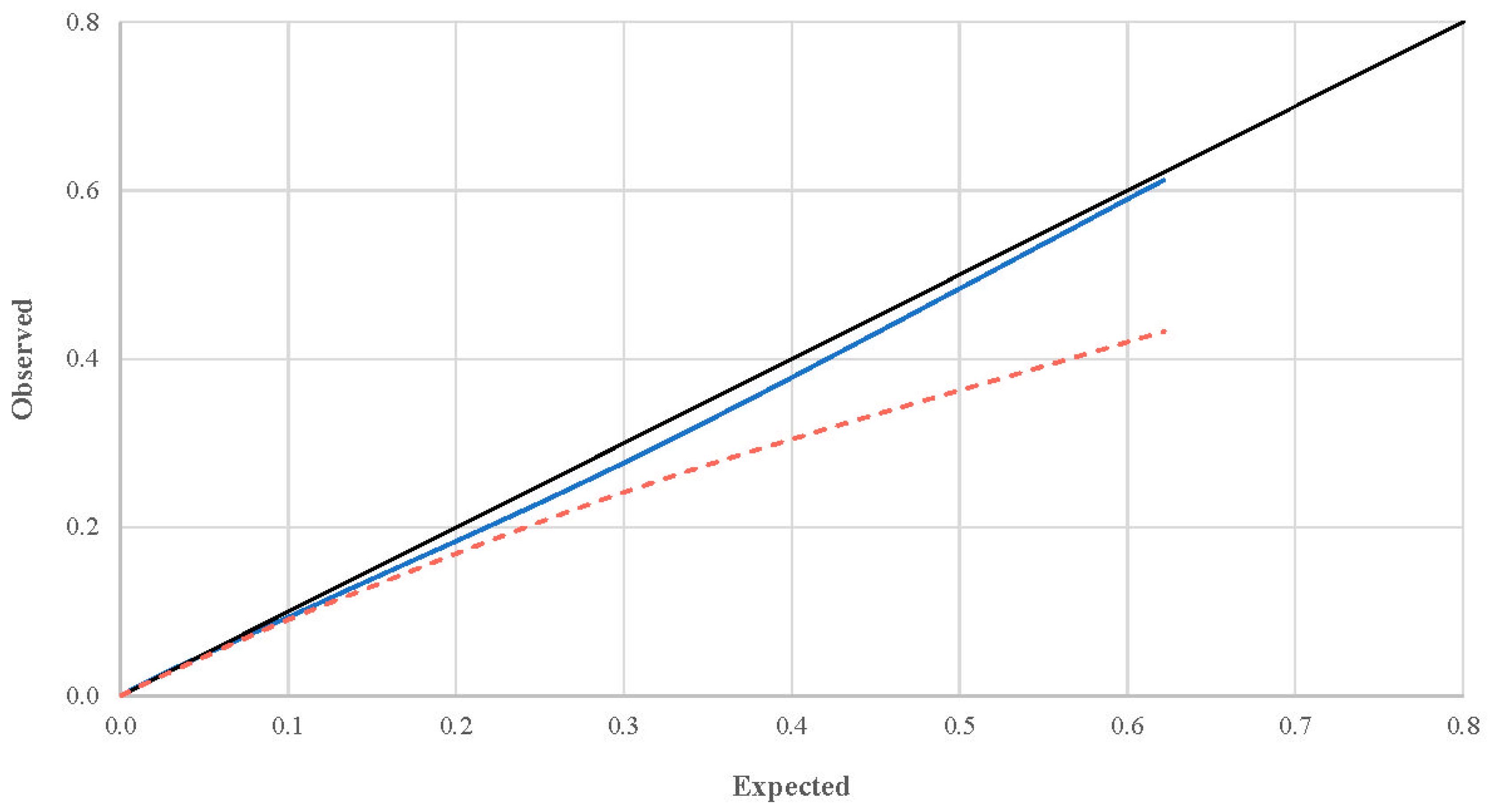
| Score | Expected Risk (%) | Internal Validation | External Validation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Absolute Frequency | Relative Frequency (%) | Cumulative Relative Frequency (%) | Observed Risk (%) | Risk Difference (%) 1 | Absolute Frequency | Relative Frequency (%) | Cumulative Relative Frequency (%) | Observed Risk (%) | Risk Difference (%) 1 | ||
| −5 | 0.00 | 162 | 0.2 | 0.2 | 0.00 | 0.00 | 127 | 0.2 | 0.2 | 0.00 | 0.00 |
| −4 | 0.00 | 7895 | 9.3 | 9.5 | 0.00 | 0.00 | 7335 | 9.1 | 9.3 | 0.00 | 0.00 |
| −3 | 0.01 | 2809 | 3.3 | 12.9 | 0.00 | 0.01 | 2662 | 3.3 | 12.6 | 0.01 | 0.00 |
| −2 | 0.03 | 30,050 | 35.6 | 48.4 | 0.02 | 0.01 | 27,660 | 34.5 | 47.1 | 0.04 | 0.00 |
| −1 | 0.12 | 9496 | 11.2 | 59.7 | 0.10 | 0.01 | 8755 | 10.9 | 58.0 | 0.12 | 0.01 |
| 0 | 0.39 | 20,779 | 24.6 | 84.2 | 0.40 | 0.01 | 20,462 | 25.5 | 83.5 | 0.40 | 0.01 |
| 1 | 1.28 | 10,869 | 12.9 | 97.1 | 1.35 | 0.07 | 10,815 | 13.5 | 96.9 | 1.25 | 0.03 |
| 2 | 4.18 | 1925 | 2.3 | 99.4 | 4.15 | 0.03 | 1977 | 2.5 | 99.4 | 3.89 | 0.28 |
| 3 | 12.75 | 471 | 0.6 | 99.9 | 11.85 | 0.90 | 446 | 0.6 | 99.9 | 11.25 | 1.50 |
| 4 | 32.90 | 39 | 0.0 | 100.0 | 30.53 | 2.37 | 46 | 0.1 | 100.0 | 26.10 | 6.81 |
| 5 | 62.19 | 7 | 0.0 | 100.0 | 61.26 | 0.93 | 3 | 0.0 | 100.0 | 43.28 | 18.91 |
| 6 | 84.66 | 0 | N/C | N/C | N/C | N/C | 0 | N/C | N/C | N/C | N/C |
| 7 | 94.87 | 0 | N/C | N/C | N/C | N/C | 0 | N/C | N/C | N/C | N/C |
| 8 | 98.42 | 0 | N/C | N/C | N/C | N/C | 0 | N/C | N/C | N/C | N/C |
| 9 | 99.52 | 0 | N/C | N/C | N/C | N/C | 0 | N/C | N/C | N/C | N/C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palazón-Bru, A.; Prieto-Castelló, M.J.; Folgado-de la Rosa, D.M.; Macanás-Martínez, A.; Mares-García, E.; Carbonell-Torregrosa, M.d.l.Á.; Gil-Guillén, V.F.; Cardona-Llorens, A.; Marhuenda-Amorós, D. Development, and Internal, and External Validation of a Scoring System to Predict 30-Day Mortality after Having a Traffic Accident Traveling by Private Car or Van: An Analysis of 164,790 Subjects and 79,664 Accidents. Int. J. Environ. Res. Public Health 2020, 17, 9518. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249518
Palazón-Bru A, Prieto-Castelló MJ, Folgado-de la Rosa DM, Macanás-Martínez A, Mares-García E, Carbonell-Torregrosa MdlÁ, Gil-Guillén VF, Cardona-Llorens A, Marhuenda-Amorós D. Development, and Internal, and External Validation of a Scoring System to Predict 30-Day Mortality after Having a Traffic Accident Traveling by Private Car or Van: An Analysis of 164,790 Subjects and 79,664 Accidents. International Journal of Environmental Research and Public Health. 2020; 17(24):9518. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249518
Chicago/Turabian StylePalazón-Bru, Antonio, María José Prieto-Castelló, David Manuel Folgado-de la Rosa, Ana Macanás-Martínez, Emma Mares-García, María de los Ángeles Carbonell-Torregrosa, Vicente Francisco Gil-Guillén, Antonio Cardona-Llorens, and Dolores Marhuenda-Amorós. 2020. "Development, and Internal, and External Validation of a Scoring System to Predict 30-Day Mortality after Having a Traffic Accident Traveling by Private Car or Van: An Analysis of 164,790 Subjects and 79,664 Accidents" International Journal of Environmental Research and Public Health 17, no. 24: 9518. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249518