
China’s Elder Care Policies 1994–2020: A Narrative Document Analysis


Abstract
:1. Introduction
Background
2. Materials and Methods
2.1. Design and Setting
2.2. Data Collection
- China’s official publicly available policy documents (in Chinese);
- Official Chinese databases: China Statistical Yearbook (in English), China’s State Council (on the Internet);
- Reports of international organizations (World Health Organization, World Bank);
- Secondary literature: search for international papers on Google Scholar, university libraries of Erasmus university and organizations worldwide.
2.3. Data Analysis
3. Results
3.1. Overview of the Five Chinese Elderly Policy Plans from 1994 until 2020
- (a)
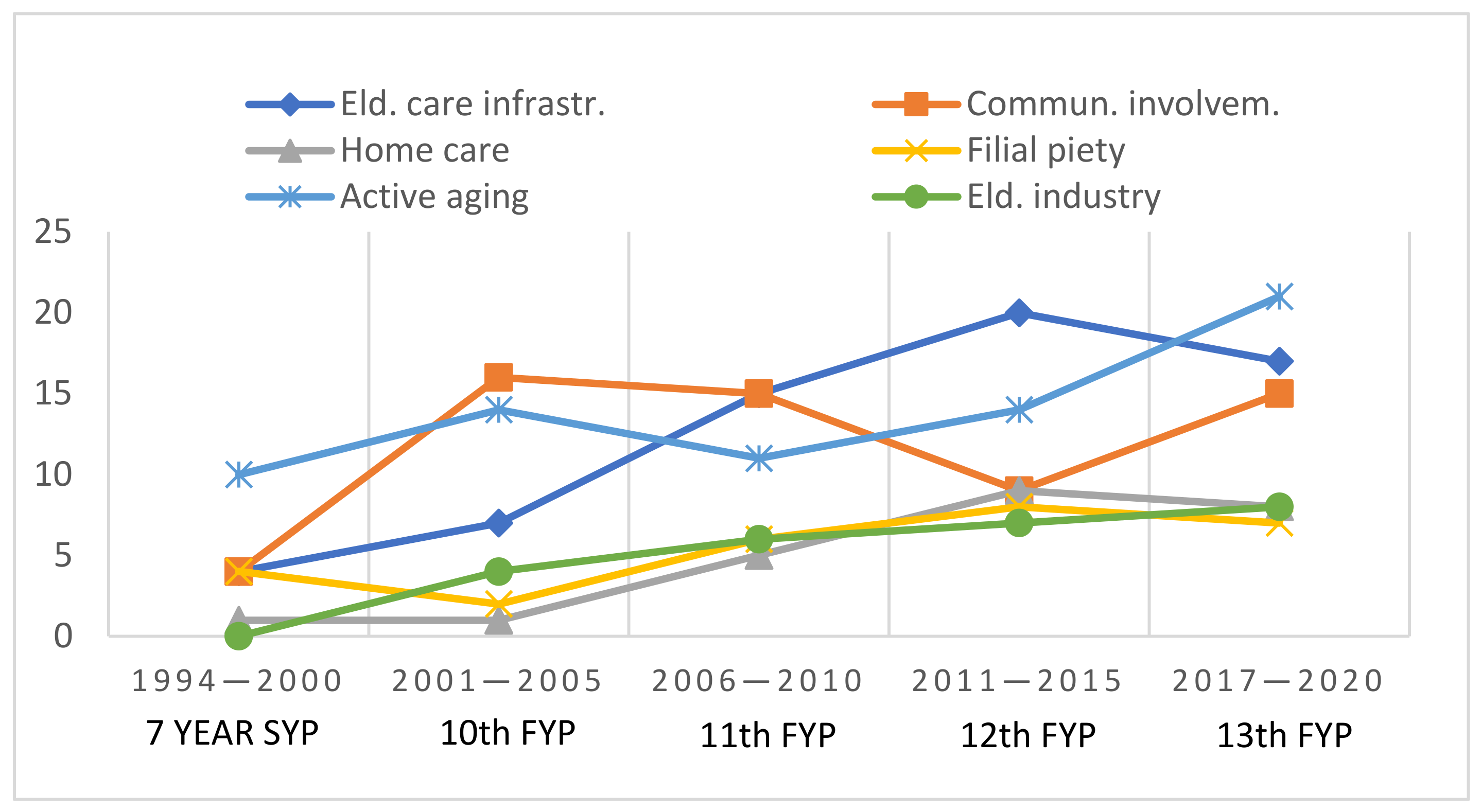
- Figure 1 provides an insight of the frequency of attention of the six themes appearing in these policies in the different time-spans.
- (b)
- Overview of China’s elderly policy plans 1994–2020.
3.2. Elderly Care Service Infrastructure
3.3. Community Care Involvement
3.4. Home-Based Care
3.5. Filial Piety
3.6. Active and Healthy Aging: ‘To Add Life to the Years That Have Been Added to Life’ (United Nations 1999)
3.7. Elderly Care Industry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Main Data of the Seventh National Population Census. Available online: http://www.stats.gov.cn/tjsj/zxfb/202105/t20210510_1817176.html (accessed on 11 May 2021).
- Glinskaya, E.; Feng, Z. Options for Aged Care in China: Building an Efficient and Sustainable Aged Care System; World Bank Publications: Washington, DC, USA, 2018. [Google Scholar]
- Feng, Z.; Liu, C.; Guan, X.; Mor, V. China’s rapidly aging population creates policy challenges in shaping a viable long-term care system. Health Aff. 2012, 31, 2764–2773. [Google Scholar] [CrossRef] [PubMed]
- Orton, M. Ageing in Urban Neighbourhoods in Beijing, China: An Ethnographic Study of Older Chinese People’s Neighbourhood Experiences. Ph.D. Thesis, Warwick University, Coventry, UK, 2017. [Google Scholar]
- Kudo, S.; Mutisya, E.; Nagao, M. Population Aging: An Emerging Research Agenda for Sustainable Development; Social Sciences: Beijing, China, 2015; pp. 940–966. [Google Scholar]
- Xu, Q.; Norstrand, J.A. Gendered Social Capital and Health Outcomes among Older Adults in China in Aging in China; Springer: Boston, MA, USA, 2012; pp. 147–168. [Google Scholar]
- Yip, W.; Hsiao, W.C. The Chinese health system at a crossroads. Health Aff. 2008, 27, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.E.; Canning, D.; Hu, L.; Liu, Y.; Mahal, A.; Yip, W. The contribution of population health and demographic change to economic growth in China and India. J. Comp. Econ. 2010, 38, 17–33. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Silverstein, M. Intergenerational social support and the psychological well- being of older parents in China. Res. Aging 2000, 22, 43–66. [Google Scholar] [CrossRef]
- Foster, L.; Walker, A. Active and successful aging: A European policy perspective. Gerontologist 2015, 55, 83–90. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Decade of Healthy Ageing: Plan of Action. In Proceedings of the 73rd World Health Assembly, Geneva, Switzerland, 17–21 May 2020. [Google Scholar]
- Tarricone, R.; Tsouros, A.D. The Solid Facts. Home Care in Europe; WHO Europe: Geneva, Switzerland, 2008. [Google Scholar]
- Kroneman, M.; Boerma, W.; Berg, M.; Groenewegen, P.; Jong, J.D.; Ginneken, E.V. The Netherlands: Health System Review. Health System in Transition; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Mattke, S.; Liu, H.; Hunter, L.E.; Gu, K.; Newberry, S. The Role of Health Care Transformation for the Chinese Dream: Powering Economic Growth, Promoting a Harmonious Society. Rand Health Q. 2014, 4, 4. [Google Scholar] [PubMed]
- Fu, H.; Li, L.; Li, M.; Yang, C.; Hsiao, W. An evaluation of systemic reforms of public hospitals: The Sanming model in China. Health Policy Plan. 2017, 32, 1135–1145. [Google Scholar] [CrossRef]
- Blumenthal, D.; Hsiao, W. Lessons from the East—China’s rapidly evolving health care system. N. Engl. J. Med. 2015, 372, 1281–1285. [Google Scholar] [CrossRef] [Green Version]
- Renard, M.F. L’économie de la Chine. No. hal-02132890. 2018. Available online: https://ideas.repec.org/p/hal/journl/hal-02132890.html (accessed on 6 January 2021).
- Litwin, H.; Lightman, E. The development of community care policy for the elder: A comparative perspective. Int. J. Health Serv. 1996, 26, 691–708. [Google Scholar] [CrossRef]
- Tang, S.; Brixi, H.; Bekedam, H. Advancing universal coverage of healthcare in China: Translating political will into policy and practice. Int. J. Health Plan. Manag. 2014, 29, 160–174. [Google Scholar] [CrossRef]
- Gu, X.Y.; Tang, S.L.; Cao, S.H. The financing and organization of health services in poor rural China: A case study in Donglan County. Int. J. Health Plan. Manag. 1995, 10, 265–282. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Sun, L. Pension reform in China. J. Aging Soc. Policy 2016, 28, 15–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, H.J.; Luo, B.; Chen, Z. Institutional Elder Care in China in Aging in China; Springer: Boston, MA, USA, 2012; pp. 221–235. [Google Scholar]
- Li, L.; Chen, Q.; Powers, D. Chinese healthcare reform: A shift toward social development. Mod. China 2012, 38, 630–645. [Google Scholar] [CrossRef]
- Urio, P. China 1949–2019: From Poverty to World Power; Springer: Boston, MA, USA, 2020. [Google Scholar]
- Proposals of the Central Committee of the Communist Party of China on Formulating the 14th Five-Year Plan for National Economic and Social Development and the Long-Term Goals for 2035, Implementation of a Gradual Extension of the Statutory Retirement Age. Available online: http://www.qstheory.cn/yaowen/2020-11/03/c_1126693429.htm (accessed on 6 January 2021).
- The Lancet Editor. Public Health in China: Achievements and future challenges. Lancet 2018, 3, 456. [Google Scholar]
- The Notification for the 13th Five-Year Plan for the National Development of the Ageing Undertaking and the Planning for the Elderly Care System Structure. Available online: http://www.gov.cn/zhengce/content/2017-03/06/content_5173930.htm (accessed on 6 January 2021).
- National Health Commission. China Health Statistical Yearbook 2020; China Union Medical University Press: Beijing, China, 2020. [Google Scholar]
- Xie, X.; Zhou, W.; Lin, L.; Fan, S.; Lin, F.; Wang, L.; Guo, T.; Ma, C.; Zhang, J.; He, Y.; et al. Internet hospitals in China: Cross-sectional survey. J. Med. Internet Res. 2017, 19, e239. [Google Scholar] [CrossRef]
- Shi, L.Y. Health care in China: A rural-urban comparison after the socioeconomic reforms. Bull. World Health Organ. 1993, 71, 723. [Google Scholar] [PubMed]
- Allen, P.; Cao, Q.; Wang, H. Public hospital autonomy in China in an international context. Int. J. Health Plan. Manag. 2014, 29, 141–159. [Google Scholar] [CrossRef]
- World Bank. China Update 2018; World Bank Report No. 132900; World Bank: Washington, DC, USA, 2018. [Google Scholar]
- Zhan, H.J.; Liu, G.; Bai, H.G. Recent development in Chinese elder homes: A reconciliation of traditional culture. Ageing Int. 2005, 30, 167–187. [Google Scholar] [CrossRef]
- China’s Elderly-Care Facility Beds More than Triple Since 2007. Available online: https://govt.chinadaily.com.cn/a/201902/09/WS5c5e6861498e27e3380381bd.html (accessed on 6 January 2021).
- Luo, B.; Zhan, H. Filial piety and functional support: Understanding intergenerational solidarity among families with migrated children in rural China. Ageing Int. 2011, 37, 69–92. [Google Scholar] [CrossRef]
- Asia Pacific Foundation of Canada. China’s Evolving Senior Care Sector. Opportunities and Challenges for Canadian Care Providers and Businesses; Asia Pacific Foundation of Canada: Vancouver, BC, Canada, 2020. [Google Scholar]
- National Health Commission. China Health Statistical Yearbook 2021; China Union Medical University Press: Beijing, China, 2021. [Google Scholar]
- Elder Care, Doctor Training among Key Issues Addressed. Available online: http://english.www.gov.cn/state_council/ministries/2018/02/06/content_281476037833892.htm (accessed on 6 January 2021).
- Zhang, Q.; Li, M.; Wu, Y. Smart home for elder care: Development and challenges in China. BMC Geriatr. 2020, 20, 318. [Google Scholar] [CrossRef]
- Hu, B.; Li, B.; Wang, J.; Shi, C. Home and community care for older people in urban China: Receipt of services and sources of payment. Health Soc. Care Community 2020, 28, 225–235. [Google Scholar] [CrossRef] [PubMed]
- China’s Development of the Ageing Undertaking of the 11th Five-Year Plan 2006–2010. Available online: http://www.scio.gov.cn/xwfbh/xwbfbh/wqfbh/2006/1212/Document/325196/325196.htm (accessed on 6 January 2021).
- China Focus: Chinese Elderly Embrace High-Quality Life. Available online: http://www.xinhuanet.com/english/2018-10/18/c_137539958.htm (accessed on 6 January 2021).
- Hu, B.; Wang, J. Unmet long-term care needs and depression: The double disadvantage of community-dwelling older people in rural China. Health Soc. Care Community 2019, 27, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Wang, F.; Li, X.; Jia, M.; Tian, M. Facilitators and barriers to implement the family doctor contracting services in China: Findings from a qualitative study. BMJ Open 2019, 9, e032444. [Google Scholar] [CrossRef] [PubMed]
- Highlights of China’s Elderly Care over Past Five Years. Available online: https://english.www.gov.cn/news/topnews/202010/29/content_WS5f9a744dc6d0f7257693e9d4.html (accessed on 6 January 2021).
- Pan, Y. Building a welfare system with Chinese characteristics: From a residual type to a moderate universalism. In Aging Welfare and Social Policy: China and the Nordic Countries in Comparative Perspective; Jing, T.K., Kuhnle, S., Pan, Y., Chen, S., Eds.; Springer: Boston, MA, USA, 2019; Volume 20. [Google Scholar]
- Xu, Q.; Chow, J.C. Exploring the community-based service delivery model: Elder care in China. Int. Soc. Work 2011, 54, 374–387. [Google Scholar]
- Chou, R.J.A. Filial piety by contract? The emergence, implementation, and implications of the “family support agreement” in China. Gerontologist 2011, 51, 3–16. [Google Scholar] [CrossRef]
- Ikels, C. Filial Piety: Practice and Discourse in Contemporary East Asia; Stanford University Press: Standford, CA, USA, 2004. [Google Scholar]
- Lin, J.Y. Rural reforms and agricultural growth in China. Am. Econ. Rev. 1992, 82, 34–51. [Google Scholar]
- Tu, M. Chinese one-child families in the age of migration: Middle-class transnational mobility, ageing parents, and the changing role of filial piety. J. Chin. Sociol. 2016, 3, 15. [Google Scholar] [CrossRef] [Green Version]
- Canda, E.R. Filial piety and care for elders: A contested Confucian virtue reexamined. J. Ethn. Cult. Divers. Soc. Work 2013, 22, 213–234. [Google Scholar] [CrossRef]
- World Health Organization. China Country Assessment Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- China to Support Couples Having Third Child. Available online: http://www.china.org.cn/china/2021-06/01/content_77538745.htm (accessed on 6 January 2021).
- Gui, T.; Koropeckyj-Cox, T. “I Am the Only Child of my Parents:” Perspectives on Future Elder Care for Parents among Chinese only-Children Living overseas. J. Cross Cult. Gerontol. 2016, 31, 255–275. [Google Scholar] [CrossRef]
- Ho, R.; Lo, P.; Chan, C.; Leung, P. An East-West approach to mind-body health of Chinese elder. In Aging in China: Implications to Social Policy 169 of a Changing Economic State, International Perspectives on Aging; Chen, S., Powell, J.L., Eds.; Springer Science + Business Media: Bostan, MA, USA, 2012. [Google Scholar]
- Naughton, B.J. The Chinese Economy: Transitions and Growth; MIT Press: Cambridge, MA, USA, 2006. [Google Scholar]
- Cheng, S.T.; Fung, H.H.; Li, L.W.; Li, T.; Woo, J.; Chi, I. Successful aging: Concepts, reflections and its relevance to Asia. In Successful Aging; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–18. [Google Scholar]
- Tan, X.; Liu, X.; Shao, H. Healthy China 2030: A vision for health care. Value Health Reg. Issues 2017, 12, 112–114. [Google Scholar] [CrossRef]
- Qiu, C. Elder Care Industry Research. In Proceedings of the Second Junior Forum on International Biomedicine and Traditional Chinese Medicine, Chengdu, China, 28 December 2018. [Google Scholar]
- Over 59 m Chinese Elderly Covered with Commercial Health Insurance. Available online: http://english.www.gov.cn/statecouncil/ministries/202002/13/content_WS5e452f91c6d0595e03c20a2b.html (accessed on 6 January 2021).
- Cao, Z.; Jing, Q. Finance for the Elder Care Industry: Business Mergers and Development Diversity. In Annual Report on Financing Old Age Care in China; Dong, K., Yao, Y., Eds.; Springer: Singapore, 2018. [Google Scholar]
- Zhang, Y. Meeting the ageing challenge: China’s social care policy for the elderly. In China Development and Governance; Wang, G., Zheng, Y., Eds.; NUS East Asian Institute: Singapore, 2012. [Google Scholar]
- The Notification of China’s Development of the Ageing Undertaking in the ‘12th Five-Year Plan 2011–2015’. Available online: http://www.gov.cn/zwgk/2011-09/23/content_1954782.htm (accessed on 6 January 2021).
- Bussolo, M.; Koettl, J.; Sinnott, E. Golden Aging: Prospects for Healthy, Active, and Prosperous Aging in Europe and Central Asia; The World Bank: Washington, DC, USA, 2015. [Google Scholar]
- Onday, O. Japan’s Society 5.0: Going beyond Industry 4.0. Bus. Eco. J. 2019, 10, 389. [Google Scholar]
- KPMG. The 14th Five-Year Plan: Sector Impact Outlook; KPMG China: Hong Kong SAR, China, 2021. [Google Scholar]
- Lin, J.Y.; Shen, Z. Reform and development strategy. In China’s 40 Years of Reform and Development; Garnaut, R., Song, L., Fang, C., Eds.; ANU Press: Canberra, Australia, 2018; p. 117. [Google Scholar]
- Sudo, K.; Kobayashi, J.; Noda, S.; Fukuda, Y.; Takahashi, K. Japan’s healthcare policy for the elderly through the concepts of self-help (Ji-jo), mutual aid (Go-jo), social solidarity care (Kyo-jo), and governmental care (Ko-jo). Biosci. Trends 2018, 12, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ney, S. Active aging policy in Europe: Between path dependency and path departure. Ageing Int. 2005, 30, 325–342. [Google Scholar] [CrossRef]
- Tu, J. From ‘Care of the Self’to ‘Entrepreneur of the Self’: Reconfiguration of Health Care Responsibilities, Needs, and Rights. In Health Care Transformation in Contemporary China; Springer: Singapore, 2019; pp. 59–84. [Google Scholar]


{kind=link}
| Policy Plan | Development Trend and Elderly Concern in the Respective Policies | Major Achievements |
|---|---|---|
| Seven Year Plan 1994–2000 | Economic level:
|
|
| 10th Five-Year Plan 2001–2005 | Economic level:
|
|
| 11th Five-Year Plan 2006–2010 | Economic level:
|
|
| 12th Five-Year Plan 2011–2015 | Economic level:
|
|
| 13th Five-Year Plan 2016–2020 | Economic level:
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krings, M.F.; van Wijngaarden, J.D.H.; Yuan, S.; Huijsman, R. China’s Elder Care Policies 1994–2020: A Narrative Document Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106141
Krings MF, van Wijngaarden JDH, Yuan S, Huijsman R. China’s Elder Care Policies 1994–2020: A Narrative Document Analysis. International Journal of Environmental Research and Public Health. 2022; 19(10):6141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106141
Chicago/Turabian StyleKrings, Marion F., Jeroen D. H. van Wijngaarden, Shasha Yuan, and Robbert Huijsman. 2022. "China’s Elder Care Policies 1994–2020: A Narrative Document Analysis" International Journal of Environmental Research and Public Health 19, no. 10: 6141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106141