
Nordic Walking Rather Than High Intensity Interval Training Reduced Myostatin Concentration More Effectively in Elderly Subjects and the Range of This Drop Was Modified by Metabolites of Vitamin D

 , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Subjects
2.3. Body Composition Assessment
2.4. Blood Collection
2.5. Applied Training Protocol
2.5.1. NW Training Protocol
2.5.2. HIIT Protocol
2.6. Statistical Calculation
3. Results
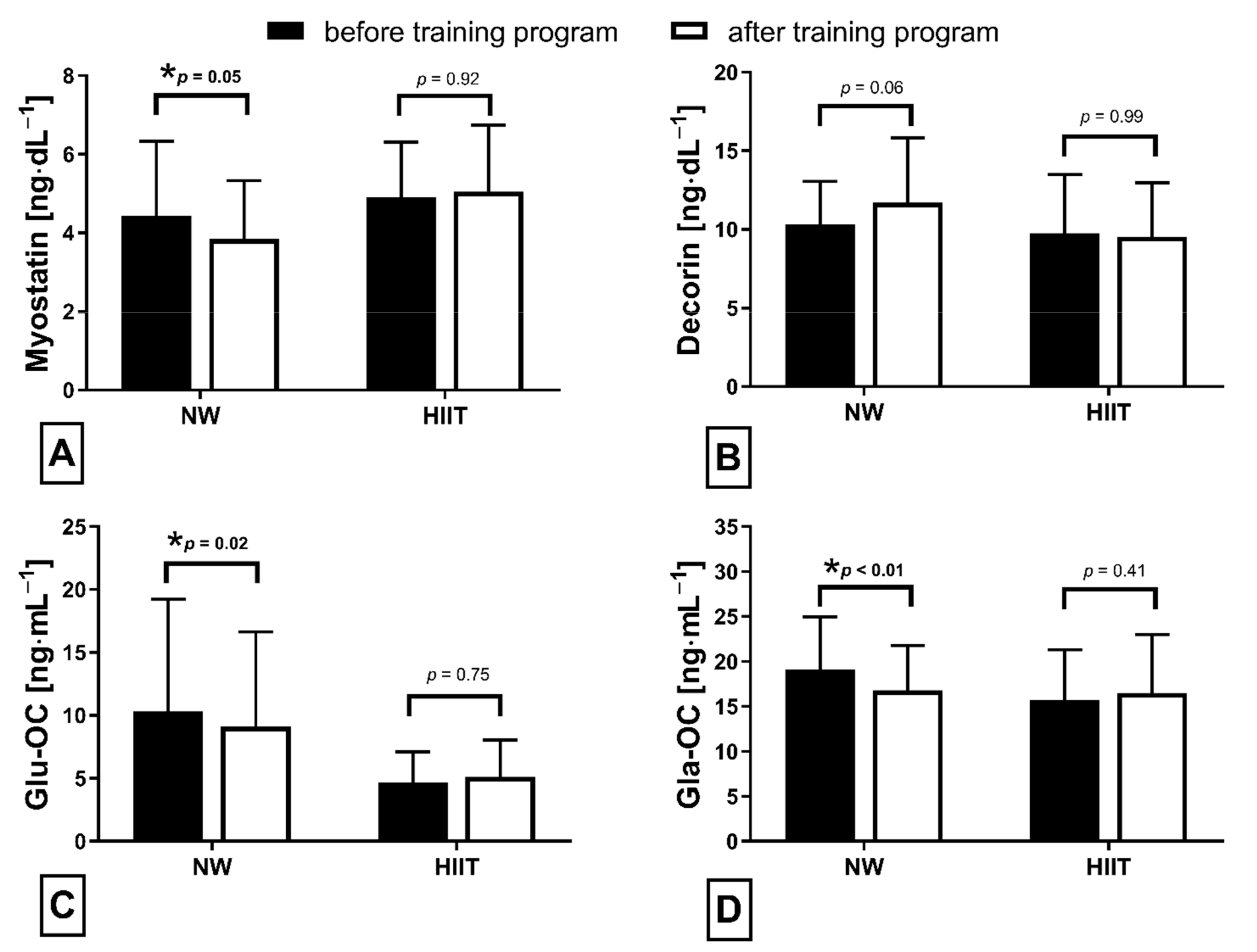
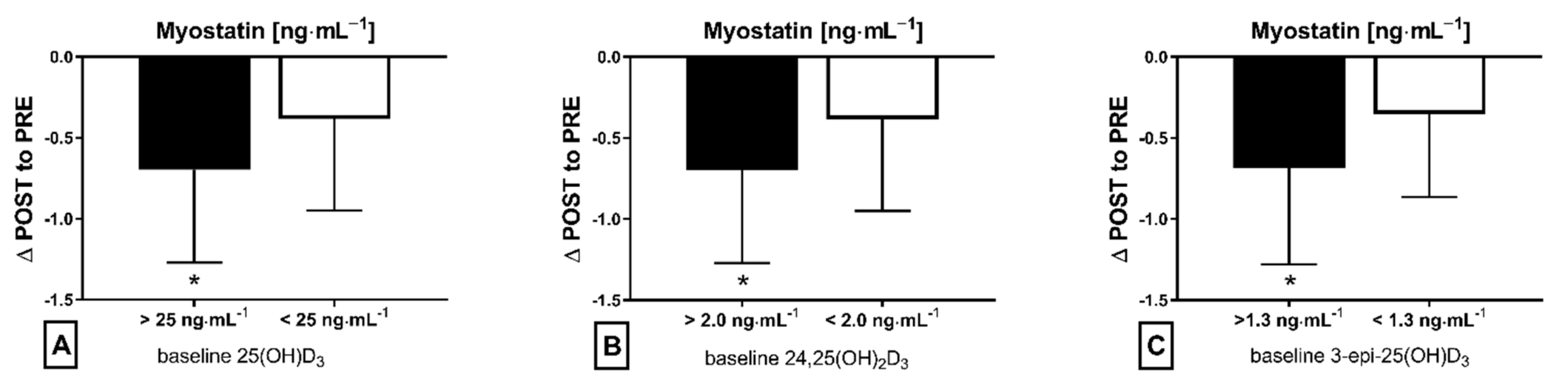
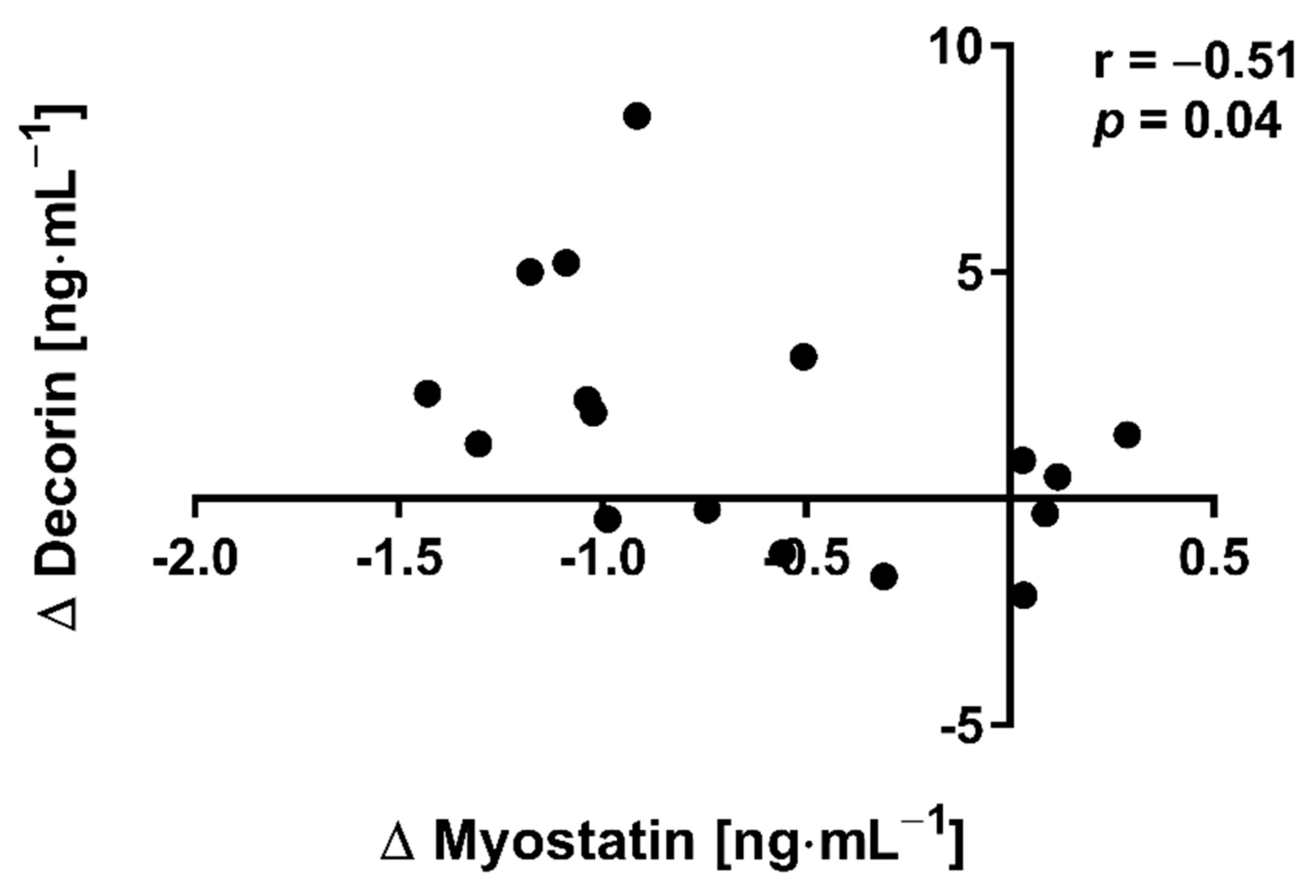
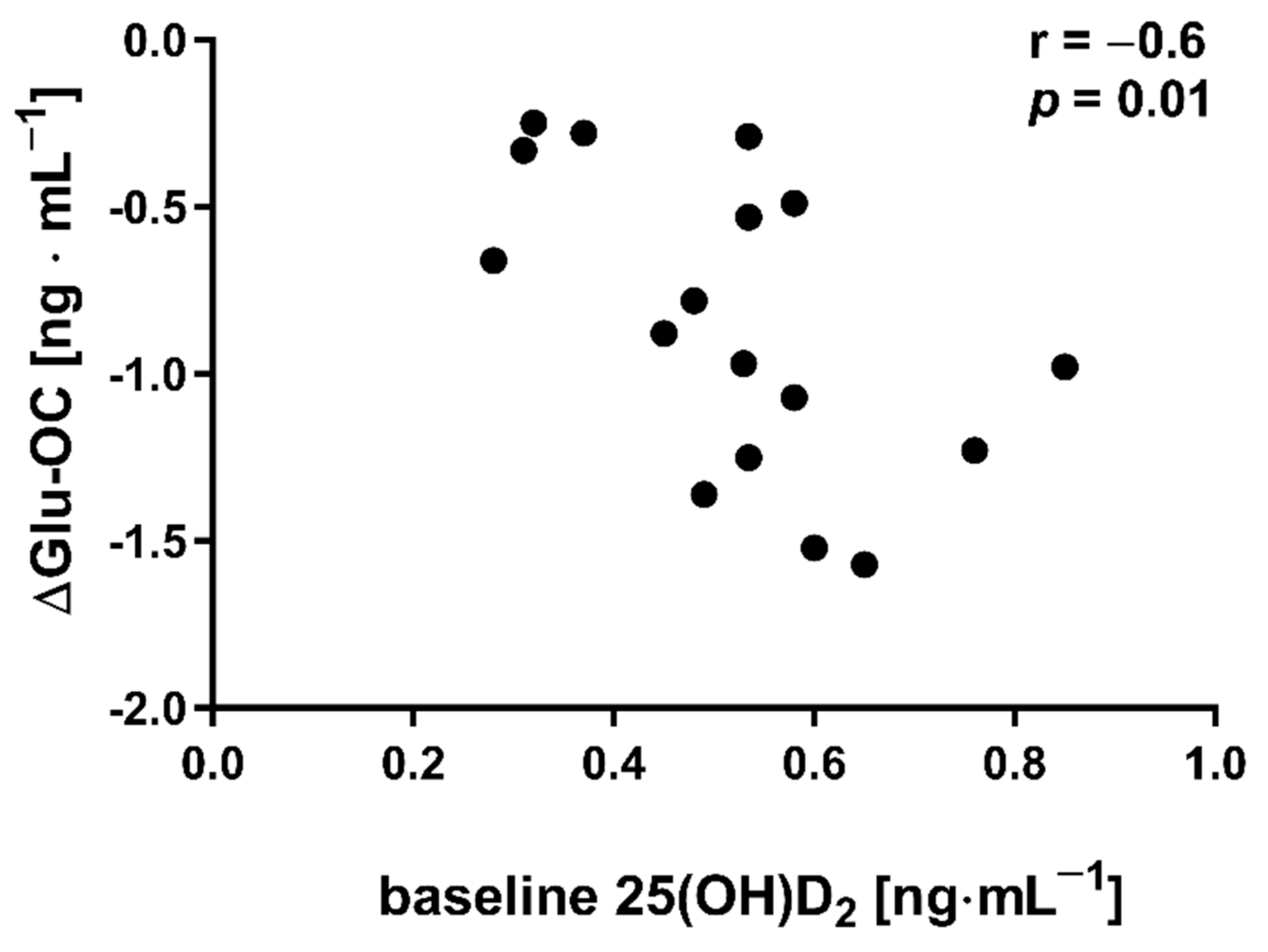
3.1. NW Trainining Program
3.2. HIIT Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ozemek, C.; Lavie, C.J.; Rognmo, O. Global physical activity levels—Need for intervention. Prog. Cardiovasc. Dis. 2019, 62, 102–107. [Google Scholar] [CrossRef]
- Zhao, R.; Bu, W.; Chen, Y.; Chen, X. The Dose-Response Associations of Sedentary Time with Chronic Diseases and the Risk for All-Cause Mortality Affected by Different Health Status: A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2020, 24, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.; Laddu, D.R.; Phillips, S.A.; Lavie, C.J.; Arena, R. A tale of two pandemics: How will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Prog. Cardiovasc. Dis. 2021, 64, 108–110. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48 440 adult patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Remelli, F.; Vitali, A.; Zurlo, A.; Volpato, S. Vitamin D Deficiency and Sarcopenia in Older Persons. Nutrients 2019, 11, 2861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbar, M.R.; Wibowo, A.; Pranata, R.; Setiabudiawan, B. Low Serum 25-hydroxyvitamin D (Vitamin D) Level Is Associated With Susceptibility to COVID-19, Severity, and Mortality: A Systematic Review and Meta-Analysis. Front. Nutr. 2021, 8, 660420. [Google Scholar] [CrossRef]
- Zemb, P.; Bergman, P.; Camargo, C.A., Jr.; Cavalier, E.; Cormier, C.; Courbebaisse, M.; Hollis, B.; Joulia, F.; Minisola, S.; Pilz, S.; et al. Vitamin D deficiency and the COVID-19 pandemic. J. Glob. Antimicrob. Resist. 2020, 22, 133–134. [Google Scholar] [CrossRef] [PubMed]
- Bullo, V.; Gobbo, S.; Vendramin, B.; Duregon, F.; Cugusi, L.; Di Blasio, A.; Bocalini, D.S.; Zaccaria, M.; Bergamin, M.; Ermolao, A. Nordic Walking Can Be Incorporated in the Exercise Prescription to Increase Aerobic Capacity, Strength, and Quality of Life for Elderly: A Systematic Review and Meta-Analysis. Rejuvenation Res. 2018, 21, 141–161. [Google Scholar] [CrossRef]
- Roy, M.; Grattard, V.; Dinet, C.; Soares, A.V.; Decavel, P.; Sagawa, Y.J. Nordic walking influence on biomechanical parameters: A systematic review. Eur. J. Phys. Rehabil. Med. 2020, 56, 607–615. [Google Scholar] [CrossRef]
- Gmiat, A.; Mieszkowski, J.; Prusik, K.; Prusik, K.; Kortas, J.; Kochanowicz, A.; Radulska, A.; Lipinski, M.; Tomczyk, M.; Jaworska, J.; et al. Changes in pro-inflammatory markers and leucine concentrations in response to Nordic Walking training combined with vitamin D supplementation in elderly women. Biogerontology 2017, 18, 535–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Z.J.; Wang, Z.Y.; Gao, H.E.; Zhou, X.F.; Li, F.H. Impact of high-intensity interval training on cardiorespiratory fitness, body composition, physical fitness, and metabolic parameters in older adults: A meta-analysis of randomized controlled trials. Exp. Gerontol. 2021, 150, 111345. [Google Scholar] [CrossRef]
- Chrois, K.M.; Dohlmann, T.L.; Sogaard, D.; Hansen, C.V.; Dela, F.; Helge, J.W.; Larsen, S. Mitochondrial adaptations to high intensity interval training in older females and males. Eur. J. Sport Sci. 2020, 20, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Garcia, J.D.; Hita-Contreras, F.; de la Torre-Cruz, M.; Fabrega-Cuadros, R.; Aibar-Almazan, A.; Cruz-Diaz, D.; Martinez-Amat, A. Risk of Falls in Healthy Older Adults: Benefits of High-Intensity Interval Training Using Lower Body Suspension Exercises. J. Aging Phys. Act. 2019, 27, 325–333. [Google Scholar] [CrossRef]
- Little, J.P.; Gillen, J.B.; Percival, M.E.; Safdar, A.; Tarnopolsky, M.A.; Punthakee, Z.; Jung, M.E.; Gibala, M.J. Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. J. Appl. Physiol. 2011, 111, 1554–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, L.D.; Elliott, B.T.; Yasar, Z.; Bampouras, T.M.; Sculthorpe, N.F.; Sanal-Hayes, N.E.M.; Hurst, C. High Intensity Interval Training (HIIT) as a Potential Countermeasure for Phenotypic Characteristics of Sarcopenia: A Scoping Review. Front. Physiol. 2021, 12, 715044. [Google Scholar] [CrossRef]
- Safdar, A.; Tarnopolsky, M.A. Exosomes as Mediators of the Systemic Adaptations to Endurance Exercise. Cold Spring Harb. Perspect. Med. 2018, 8, a029827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanzleiter, T.; Rath, M.; Gorgens, S.W.; Jensen, J.; Tangen, D.S.; Kolnes, A.J.; Kolnes, K.J.; Lee, S.; Eckel, J.; Schurmann, A.; et al. The myokine decorin is regulated by contraction and involved in muscle hypertrophy. Biochem. Biophys. Res. Commun. 2014, 450, 1089–1094. [Google Scholar] [CrossRef]
- Micielska, K.; Gmiat, A.; Zychowska, M.; Kozlowska, M.; Walentukiewicz, A.; Lysak-Radomska, A.; Jaworska, J.; Rodziewicz, E.; Duda-Biernacka, B.; Ziemann, E. The beneficial effects of 15 units of high-intensity circuit training in women is modified by age, baseline insulin resistance and physical capacity. Diabetes Res. Clin. Pract. 2019, 152, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Miura, T.; Kishioka, Y.; Wakamatsu, J.; Hattori, A.; Hennebry, A.; Berry, C.J.; Sharma, M.; Kambadur, R.; Nishimura, T. Decorin binds myostatin and modulates its activity to muscle cells. Biochem. Biophys. Res. Commun. 2006, 340, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Baczek, J.; Silkiewicz, M.; Wojszel, Z.B. Myostatin as a Biomarker of Muscle Wasting and other Pathologies-State of the Art and Knowledge Gaps. Nutrients 2020, 12, 2401. [Google Scholar] [CrossRef] [PubMed]
- Mera, P.; Laue, K.; Ferron, M.; Confavreux, C.; Wei, J.; Galan-Diez, M.; Lacampagne, A.; Mitchell, S.J.; Mattison, J.A.; Chen, Y.; et al. Osteocalcin Signaling in Myofibers Is Necessary and Sufficient for Optimum Adaptation to Exercise. Cell Metab. 2016, 23, 1078–1092. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Real, J.M.; Izquierdo, M.; Ortega, F.; Gorostiaga, E.; Gomez-Ambrosi, J.; Moreno-Navarrete, J.M.; Fruhbeck, G.; Martinez, C.; Idoate, F.; Salvador, J.; et al. The relationship of serum osteocalcin concentration to insulin secretion, sensitivity, and disposal with hypocaloric diet and resistance training. J. Clin. Endocrinol. Metab. 2009, 94, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Zoch, M.L.; Clemens, T.L.; Riddle, R.C. New insights into the biology of osteocalcin. Bone 2016, 82, 42–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, N.K.; Sowa, H.; Hinoi, E.; Ferron, M.; Ahn, J.D.; Confavreux, C.; Dacquin, R.; Mee, P.J.; McKee, M.D.; Jung, D.Y.; et al. Endocrine regulation of energy metabolism by the skeleton. Cell 2007, 130, 456–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auyeung, T.W.; Lee, J.S.; Leung, J.; Kwok, T.; Woo, J. Adiposity to muscle ratio predicts incident physical limitation in a cohort of 3,153 older adults--an alternative measurement of sarcopenia and sarcopenic obesity. Age 2013, 35, 1377–1385. [Google Scholar] [CrossRef] [Green Version]
- Volgyi, E.; Tylavsky, F.A.; Lyytikainen, A.; Suominen, H.; Alen, M.; Cheng, S. Assessing body composition with DXA and bioimpedance: Effects of obesity, physical activity, and age. Obesity 2008, 16, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.; Nambi, S.S.; Mather, K.; Baron, A.D.; Follmann, D.A.; Sullivan, G.; Quon, M.J. Quantitative insulin sensitivity check index: A simple, accurate method for assessing insulin sensitivity in humans. J. Clin. Endocrinol. Metab. 2000, 85, 2402–2410. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Mieszkowski, J.; Stankiewicz, B.; Kochanowicz, A.; Niespodzinski, B.; Kowalik, T.; Zmijewski, M.; Kowalski, K.; Rola, R.; Bienkowski, T.; Antosiewicz, J. Ultra-Marathon-Induced Increase in Serum Levels of Vitamin D Metabolites: A Double-Blind Randomized Controlled Trial. Nutrients 2020, 12, 3629. [Google Scholar] [CrossRef] [PubMed]
- Kortas, J.; Prusik, K.; Flis, D.; Prusik, K.; Ziemann, E.; Leaver, N.; Antosiewicz, J. Effect of Nordic Walking training on iron metabolism in elderly women. Clin. Interv. Aging 2015, 10, 1889–1896. [Google Scholar] [CrossRef] [Green Version]
- Kortas, J.; Ziemann, E.; Juszczak, D.; Micielska, K.; Kozlowska, M.; Prusik, K.; Prusik, K.; Antosiewicz, J. Iron Status in Elderly Women Impacts Myostatin, Adiponectin and Osteocalcin Levels Induced by Nordic Walking Training. Nutrients 2020, 12, 1129. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Kalantar-Zadeh, K.; Anker, S.D. COVID-19: A major cause of cachexia and sarcopenia? J. Cachexia Sarcopenia Muscle 2020, 11, 863–865. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Dantas Damascena, A.; Galvao Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Koundourakis, N.E.; Avgoustinaki, P.D.; Malliaraki, N.; Margioris, A.N. Muscular effects of vitamin D in young athletes and non-athletes and in the elderly. Hormones 2016, 15, 471–488. [Google Scholar] [CrossRef] [Green Version]
- Kwon, J.H.; Moon, K.M.; Min, K.W. Exercise-Induced Myokines can Explain the Importance of Physical Activity in the Elderly: An Overview. Healthcare 2020, 8, 378. [Google Scholar] [CrossRef] [PubMed]
- Knuiman, P.; Hopman, M.T.E.; Hangelbroek, R.; Mensink, M. Plasma cytokine responses to resistance exercise with different nutrient availability on a concurrent exercise day in trained healthy males. Physiol. Rep. 2018, 6, e13708. [Google Scholar] [CrossRef]
- Gubbiotti, M.A.; Vallet, S.D.; Ricard-Blum, S.; Iozzo, R.V. Decorin interacting network: A comprehensive analysis of decorin-binding partners and their versatile functions. Matrix Biol. J. Int. Soc. Matrix Biol. 2016, 55, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Araki, K.; Wakabayashi, H.; Shintani, K.; Morikawa, J.; Matsumine, A.; Kusuzaki, K.; Sudo, A.; Uchida, A. Decorin suppresses bone metastasis in a breast cancer cell line. Oncology 2009, 77, 92–99. [Google Scholar] [CrossRef]
- Hittel, D.S.; Berggren, J.R.; Shearer, J.; Boyle, K.; Houmard, J.A. Increased secretion and expression of myostatin in skeletal muscle from extremely obese women. Diabetes 2009, 58, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Amor, M.; Itariu, B.K.; Moreno-Viedma, V.; Keindl, M.; Jurets, A.; Prager, G.; Langer, F.; Grablowitz, V.; Zeyda, M.; Stulnig, T.M. Serum Myostatin is Upregulated in Obesity and Correlates with Insulin Resistance in Humans. Exp. Clin. Endocrinol. Diabetes Off. J. Ger. Soc. Endocrinol. Ger. Diabetes Assoc. 2019, 127, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Ahn, N.; Kim, K. Effects of 12-week exercise training on osteocalcin, high-sensitivity C-reactive protein concentrations, and insulin resistance in elderly females with osteoporosis. J. Phys. Ther. Sci. 2016, 28, 2227–2231. [Google Scholar] [CrossRef] [Green Version]
- Wieczorek-Baranowska, A.; Nowak, A.; Pilaczynska-Szczesniak, L. Osteocalcin and glucose metabolism in postmenopausal women subjected to aerobic training program for 8 weeks. Metab. Clin. Exp. 2012, 61, 542–545. [Google Scholar] [CrossRef]
- Levinger, I.; Jerums, G.; Stepto, N.K.; Parker, L.; Serpiello, F.R.; McConell, G.K.; Anderson, M.; Hare, D.L.; Byrnes, E.; Ebeling, P.R.; et al. The effect of acute exercise on undercarboxylated osteocalcin and insulin sensitivity in obese men. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2014, 29, 2571–2576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Huenchullan, S.F.; Maharjan, B.R.; Williams, P.F.; Tam, C.S.; McLennan, S.V.; Twigg, S.M. Skeletal muscle adiponectin induction depends on diet, muscle type/activity, and exercise modality in C57BL/6 mice. Physiol. Rep. 2018, 6, e13848. [Google Scholar] [CrossRef]
- Gibala, M.J.; Jones, A.M. Physiological and performance adaptations to high-intensity interval training. Nestle Nutr. Inst. Workshop Ser. 2013, 76, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batacan, R.B., Jr.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Shaban, N.; Kenno, K.A.; Milne, K.J. The effects of a 2 week modified high intensity interval training program on the homeostatic model of insulin resistance (HOMA-IR) in adults with type 2 diabetes. J. Sports Med. Phys. Fit. 2014, 54, 203–209. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NW (n = 18) | HIIT (n =14) | rANOVA | |||
|---|---|---|---|---|---|
| I | II | I | II | Group × Time Interaction | |
| Sarcopenic Obesity Indicators | |||||
| BF/FFM [kg⋅kg−1] | 0.47 + 0.17 | 0.47 + 0.16 | 0.51 ± 0.18 | 0.50 ± 0.19 | 0.28 |
| BM/FFM [kg⋅kg−1] | 1.47 + 0.17 | 1.47 + 0.16 | 1.51 ± 0.18 | 1.50 ± 0.19 | 0.28 |
| NW (n = 18) | HIIT (n = 14) | rANOVA | |||
|---|---|---|---|---|---|
| I | II | I | II | Group × Time Interaction | |
| Glucose homeostasis indicators | |||||
| Glucose [mg⋅dL−1] | 100.83 ± 21.92 | 93.69 ± 6.01 | 100.36 ± 8.70 | 96.29 ± 8.88 | 0.73 |
| Insulin [µIU⋅mL−1] | 7.80 ± 4.87 | 8.19 ± 4.15 | 7.92 ± 4.90 | 8.19 ± 6.02 | 0.62 |
| QUICKI | 0.359 ± 0.04 | 0.357 ± 0.03 | 0.358 ± 0.04 | 0.362 ± 0.04 | 0.42 |
| HOMA-IR | 2.02 ± 1.51 | 1.88 ± 1.10 | 2.02 ± 1.38 | 2.01 ± 1.64 | 0.48 |
| Lipid profile | |||||
| Total cholesterol [mg⋅dL−1] | 232.50 ± 35.05 | 231.06 ± 35.68 | 178.93 ± 43.71 | 176.86 ± 31.34 | 0.94 |
| HDL cholesterol [mg⋅dL−1] | 77.75 ± 29.39 | 73.75 ± 20.43 | 54.45 ± 15.52 | 54.79 ± 15.27 | 0.27 |
| LDL cholesterol [mg⋅dL−1] | 133.44 ± 37.36 | 133.5 ± 41.35 | 104.94 ± 35.48 | 101.71 ± 28.21 | 0.63 |
| Triglycerides [mg⋅dL−1] | 105.63 ± 35.34 | 118.75 ± 39.74 | 97.07 ± 61.73 | 101.43 ± 44.04 | 0.54 |
| Vitamin D metabolites | |||||
| 25(OH)D3 [ng⋅mL−1] | 27.61 ± 10.82 | 27.78 ± 7.86 | 23.8 ± 5.18 | 25.54 ± 7.06 | 0.21 |
| 25(OH)D2 [ng⋅mL−1] | 0.52 ± 0.15 | 0.47 ± 0.11 | 0.44 ± 0.16 | 0.45 ± 0.15 | 0.08 |
| 24,25(OH)2D3 [ng⋅mL−1] | 2.62 ± 1.59 | 2.68 ± 1.43 | 2.12 ± 0.71 | 2.16 ± 0.83 | 0.94 |
| 3-epi-25(OH)D3 [ng⋅mL−1] | 1.34 ± 0.59 | 1.61 ± 0.68 | 1.23 ± 0.41 | 1.37 ± 0.63 | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Micielska, K.; Flis, M.; Kortas, J.A.; Rodziewicz-Flis, E.; Antosiewicz, J.; Wochna, K.; Lombardi, G.; Ziemann, E. Nordic Walking Rather Than High Intensity Interval Training Reduced Myostatin Concentration More Effectively in Elderly Subjects and the Range of This Drop Was Modified by Metabolites of Vitamin D. Nutrients 2021, 13, 4393. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124393
Micielska K, Flis M, Kortas JA, Rodziewicz-Flis E, Antosiewicz J, Wochna K, Lombardi G, Ziemann E. Nordic Walking Rather Than High Intensity Interval Training Reduced Myostatin Concentration More Effectively in Elderly Subjects and the Range of This Drop Was Modified by Metabolites of Vitamin D. Nutrients. 2021; 13(12):4393. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124393
Chicago/Turabian StyleMicielska, Katarzyna, Marta Flis, Jakub Antoni Kortas, Ewa Rodziewicz-Flis, Jędrzej Antosiewicz, Krystian Wochna, Giovanni Lombardi, and Ewa Ziemann. 2021. "Nordic Walking Rather Than High Intensity Interval Training Reduced Myostatin Concentration More Effectively in Elderly Subjects and the Range of This Drop Was Modified by Metabolites of Vitamin D" Nutrients 13, no. 12: 4393. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124393