
Migraine and Its Association with Hyperactivity of Cell Membranes in the Course of Latent Magnesium Deficiency—Preliminary Study of the Importance of the Latent Tetany Presence in the Migraine Pathogenesis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Groups
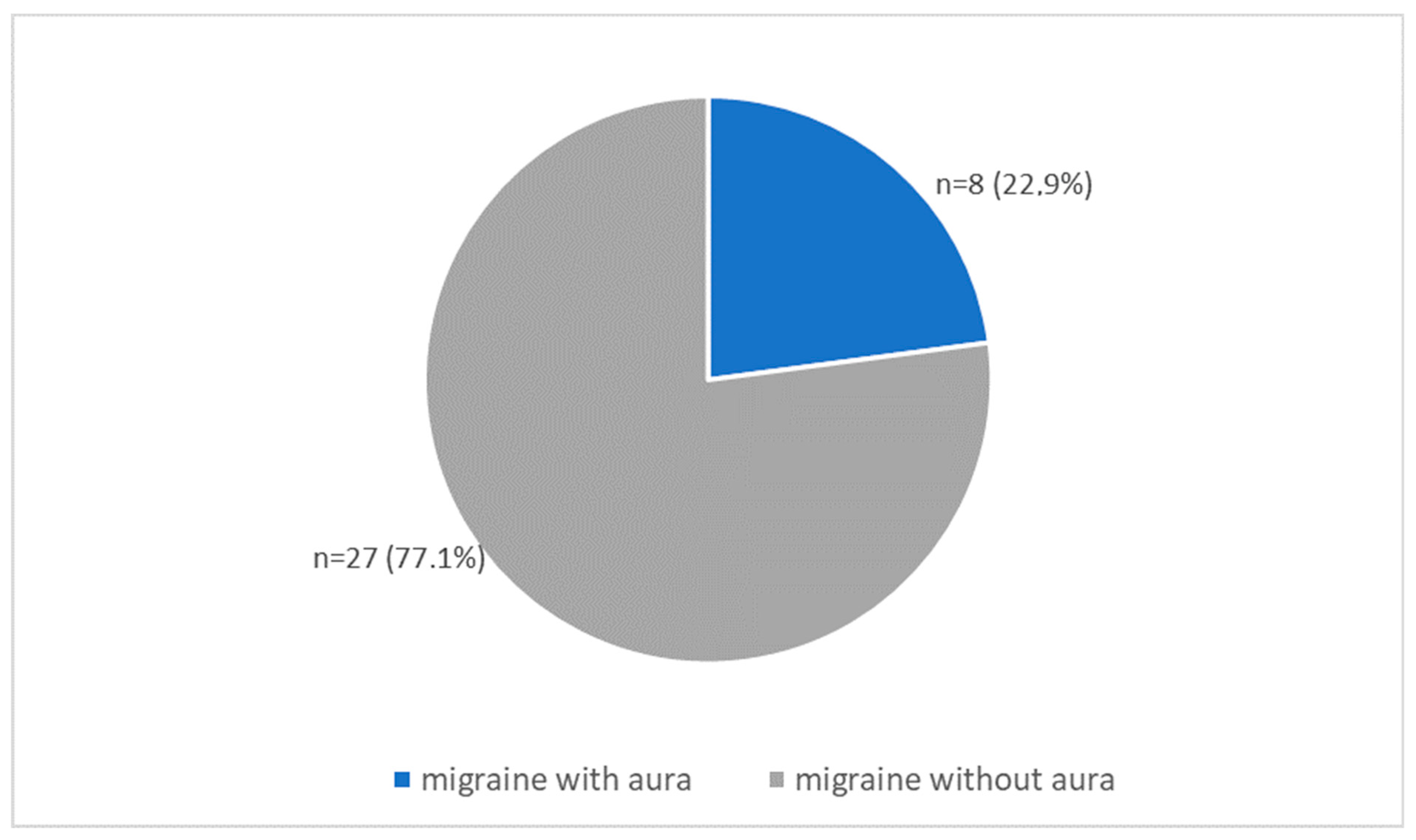
2.1.1. Study Group with Migraine
2.1.2. Control Group
2.2. Clinical Research
2.3. Statistical Analysis
3. Results
3.1. Demographic Data of Both Group: Migraine vs. Control
3.1.1. Sex in Migraine Group vs. Controls
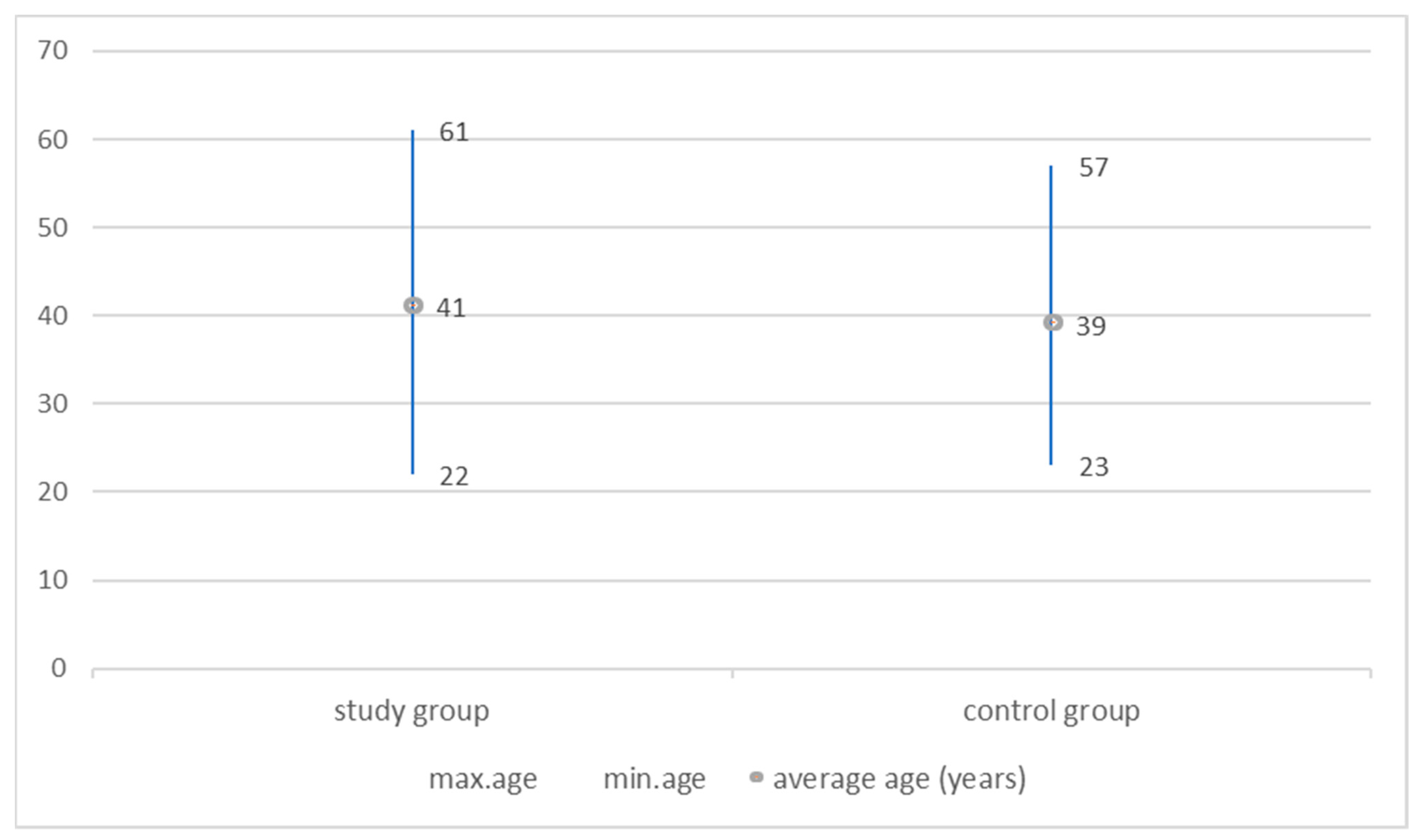
3.1.2. Age in Migraine Group vs. Controls
3.2. Comparison of Tetany Test Results between Groups
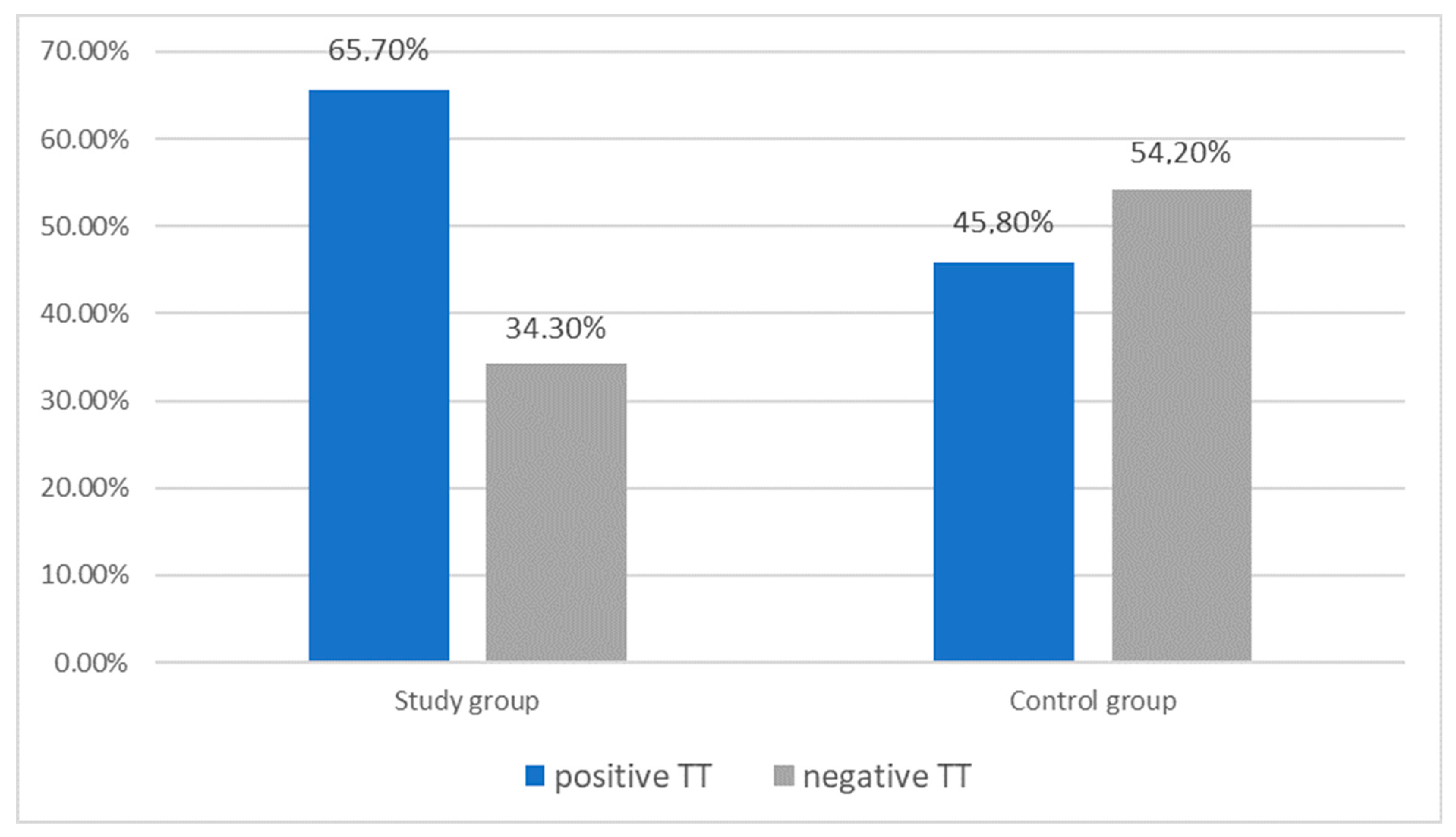
3.2.1. Tetany Test Results: Migraine Group vs. Controls
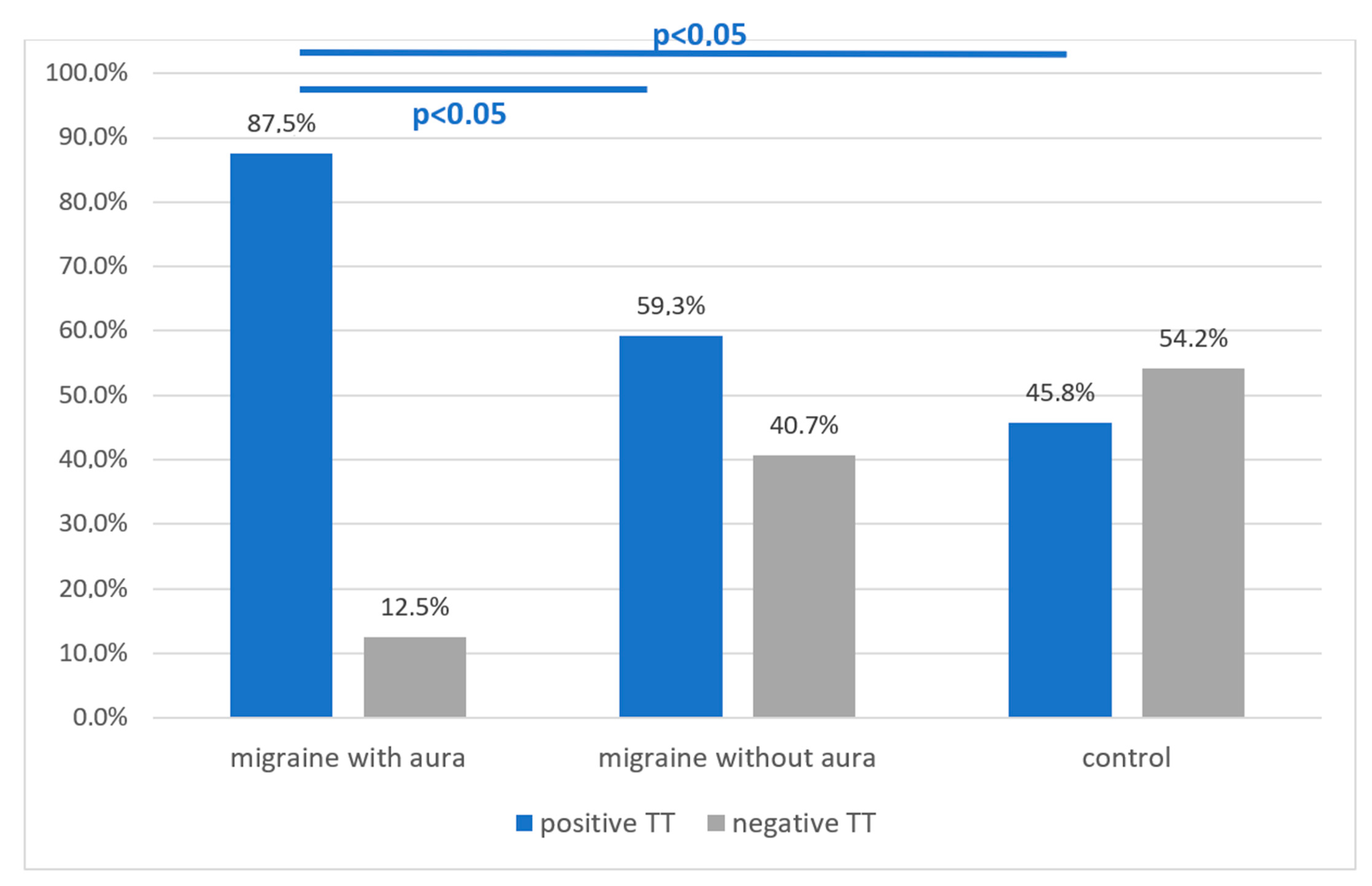
3.2.2. Tetany Test Results: Migraine Subgroup with Aura vs. without Aura vs. Control Group
3.3. Demographic Data of Migraine Group vs. Tetany Test
3.3.1. Sex in Migraine Group vs. Tetany Test Result
3.3.2. Sex in Migraine Subgroups vs. Tetany Test Result
3.3.3. Age vs. Tetany Test in Migraine Group
3.4. Tetany Test Results vs. Clinical Data in the Migraine Group
3.4.1. Tetany Test Results vs. the Frequency of Migraine Attacks
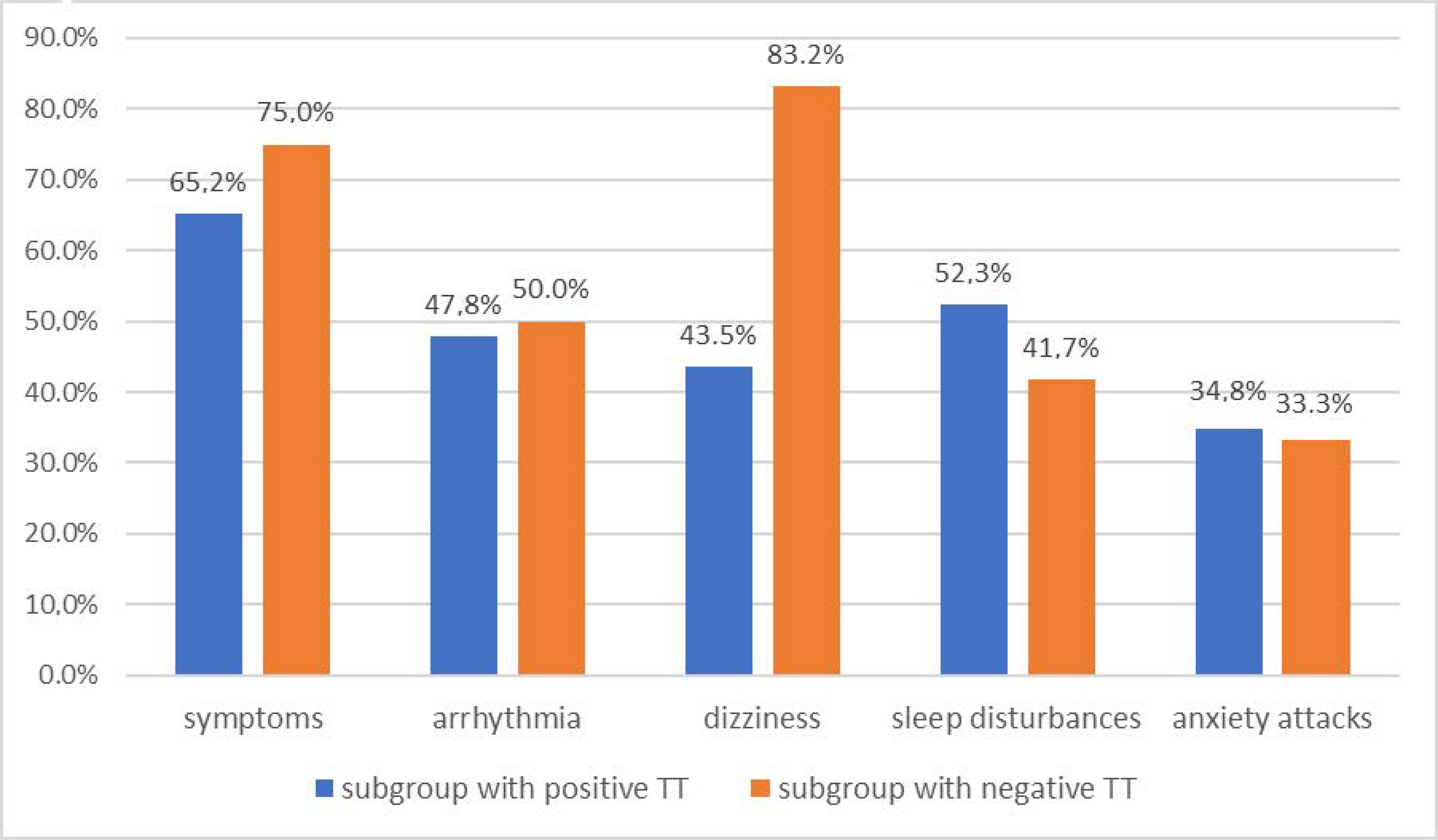
3.4.2. Tetany Test Results vs. Incidence of General Complaints in the Migraine Group
3.4.3. Tetany Test Results vs. Cardiac Arrhythmia in the Migraine Group
3.4.4. Tetany Test Results vs. Dizziness in the Migraine Group
3.4.5. Tetany Test Results vs. Sleep Disturbances in the Migraine Group
3.4.6. Tetany Test Results vs. Anxiety Attacks in the Migraine Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salomone, S.; Caraci, F.; Capasso, A. Migraine: An Overview. Open Neurol. J. 2009, 3, 64–71. [Google Scholar] [CrossRef]
- Hoffmann, J.; Charles, A. Glutamate and Its Receptors as Therapeutic Targets for Migraine. Neurotherapeutics 2018, 15, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Goadsby, P.J.; Holland, P.R. Pathophysiology of Migraine: An Update. Neurol. Clin. 2019, 37, 651–671. [Google Scholar] [CrossRef]
- Olesen, J.; Larsen, B.; Lauritzen, M. Focal Hyperemia Followed by Spreading Oligemia and Impaired Activation of rCBF in Classic Migraine. Ann. Neurol. 1981, 9, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. Pathophysiology of migraine. In Migraine in General Practice; Ekbom, K., Ed.; Smith-Gordon: London, UK, 1993. [Google Scholar]
- Andersen, A.R.; Friberg, L.; Olesen, T.; Olesen, J. Delayed Hyperemia Following Hypoperfusion in Classic Migraine. Single Photon Emission Computed Tomographic Demonstration. Arch. Neurol. 1988, 45, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Choudhuri, R.; Cui, L.; Young, C.; Bower, S.; Klein, R.M.; Welch, K.M.; Berman, N. Cortical Spreading Depression and Gene Regulation: Revalance to Migraine. Ann. Neurol. 2002, 51, 499–506. [Google Scholar] [CrossRef]
- Zanette, E.M.; Angoli, A.; Roberti, C.; Chiarotti, F.; Cerbo, R.; Fieschi, C. Transcranial Doppler in Spontaneus Attacks of Migraine. Stroke 1992, 23, 680–685. [Google Scholar] [CrossRef] [Green Version]
- Woods, R.P.; Jacoboni, M.; Mazziotta, J.C. Bilateral spreading cerebral hypoperfusion during spontaneous migraine headache. N. Engl. J. Med. 1994, 331, 1689–1692. [Google Scholar] [CrossRef]
- O’Brien, M.D. Spreading Cerebral Hypoperfusion during Migraine Headache. N. Engl. J. Med. 1995, 332, 1516–1518. [Google Scholar]
- Lindahl, A.J.; Allder, S.; Jefferson, D.; Moody, A.; Martel, A. Prolonged hemiplegic migraine associated with unilateral hyperperfusion on perfusion weighted magnetic resonance imaging. J. Neurol. Neurosurg. Psychiatry 2002, 73, 202–203. [Google Scholar] [CrossRef] [Green Version]
- Vinogradova, L.V. Initiation of spreading depression by synaptic and network hyperactivity: Insights into trigger mechanisms of migraine aura. Cephalalgia 2018, 38, 1177–1187. [Google Scholar] [CrossRef] [PubMed]
- van Harreveld, A.; Stamm, J.S.; Christensen, E. Spreading depression in rabbit, cat and monkey. Am. J. Physiol. 1956, 184, 312–320. [Google Scholar] [CrossRef] [Green Version]
- Olesen, J. Understanding the biologic basis of migraine. N. Engl. J. Med. 1994, 331, 1713–1714. [Google Scholar] [CrossRef]
- Martens-Mantai, T.; Speckmann, E.J.; Gorji, A. Propagation of cortical spreading depression into the hippocampus: The role of the entorhinal cortex. Synapse 2014, 68, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Boska, M.D.; Welch, K.M.A.; Barker, P.B.; Nelson, J.A.; Schultz, L. Contrasts in cortical magnesium, phospholipid and energy metabolism between migraine syndromes. Neurology 2002, 58, 1227–1233. [Google Scholar] [CrossRef]
- Mishima, K.; Takeshima, T.; Shimomura, T.; Okada, H.; Kitano, A.; Takahashi, K.; Nakashima, K. Platelet Jonized Magnezium, Cyclic AMP, and Cyclic GMP Levels in Migraine and Tension-Type Headache. Headache 1997, 37, 561–564. [Google Scholar] [CrossRef]
- Chang, C.L.; Donaghy, M.; Poulter, N. Migraine and stroke in young women: Case-control study. BMJ 1999, 318, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Brennan, K.C.; Beltran-Parazal, L.; Lopez-Valdez, H.E.; Theriot, J.; Toga, A.W.; Charles, A.C. Distinct vascular conduction with cortical spreading depression. J. Neuropsiol. 2007, 97, 4143–4151. [Google Scholar] [CrossRef]
- Lauritzen, M. Cortical spreading depression in migraine. Cephalalgia 2001, 21, 757–760. [Google Scholar] [CrossRef]
- Sanchez del Rio, M.; Olesen, J.; Diener, H.C. Hemodynamics and neuroimaging of migraines. In The Headaches, 3rd ed.; Olesen, J., Goadsby, P.J., Ramadan, N.M., Tfel-Hansen, P., Welch, K.M.A., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 351–361. [Google Scholar]
- Dolati, S.; Rikhtegar, R.; Mehdizadeh, A.; Yousefi, M. The Role of Magnesium in Pathophysiology and Migraine Treatment. Biol. Trace Elem. Res. 2019. [Google Scholar] [CrossRef]
- Kirkland, A.E.; Sarlo, G.L.; Holton, K.F. The Role of Magnesium in Neurological Disorders. Nutrients 2018, 10, 730. [Google Scholar] [CrossRef] [Green Version]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Adelman, W.J. The effect of external calcium and magnesium depletion on single nerve fibers. J. Gen. Physiol. 1956, 39, 753–772. [Google Scholar] [CrossRef] [Green Version]
- Swaminathan, R. Magnesium Metabolism and its Disorders. Clin. Biochem. Rev. 2003, 24, 47–66. [Google Scholar]
- Faheemuddin, A.; Abdul, M. Magnesium: The Forgotten Electrolyte—A Review on Hypomagnesemia. Med. Sci. 2019, 7, 56. [Google Scholar] [CrossRef] [Green Version]
- Vizinová, H.; Bartousek, J.; Bartek, J. Magnesium balance in patients with spasmophilia. Relation to results of electromyography. Cas. Lek. Cesk. 1997, 136, 448–450. [Google Scholar]
- Seelig, M.S.; Berger, A.R.; Spielholz, N. Latent tetany and anxiety, marginal magnesium deficit, and normocalcemia. Dis. Nerv. Syst. 1975, 36, 461–465. [Google Scholar] [PubMed]
- Durlach, J.; Bac, P.; Durlach, V.; Bara, M.; Guiet-Bara, A. Neurotic, neuromuscular and autonomic nervous form of magnesium imbalance. Magnes. Res. 1997, 10, 169–195. [Google Scholar]
- Mauskop, A.; Altura, B.T.; Altura, B.M. Serum Ionized Magnesium Levels and Serum Ionized Calcium/Ionized Magnesium Ratios in Women With Menstrual Migraine. Headache 2002, 42, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Welch, K.M.; Ramadan, N.M. Mitochondria, magnesium and migraine. J. Neurol. Sci. 1995, 134, 9–14. [Google Scholar] [CrossRef]
- Ramadan, N.M.; Halvorson, H.; Vende-Linde, A.; Levine, S.R.; Helpern, J.A.; Welch, K.M.A. Low brain magnesium in migraine. Headache 1989, 29, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Aloisi, P.; Marrelli, A.; Porto, C.; Tozzi, E.; Cerone, G. Visual Evoked Potentials and Serum Magnesium Levels in Juvenile Migraine Patients. Headache 1997, 37, 383–385. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age (Year) | Sex | Type of Migraine | Seizure Frequency | Tetany Test |
|---|---|---|---|---|---|
| 1 | 37 | M | B | 1 | 1 |
| 2 | 40 | F | B | 1 | 1 |
| 3 | 44 | M | B | 1 | 1 |
| 4 | 34 | F | A | 1 | 1 |
| 5 | 57 | F | A | 1 | 1 |
| 6 | 33 | F | B | 2 | 1 |
| 7 | 56 | F | B | 1 | 1 |
| 8 | 38 | F | A | 1 | 1 |
| 9 | 47 | F | B | 1 | 1 |
| 10 | 23 | F | B | 2 | 1 |
| 11 | 37 | F | B | 1 | 1 |
| 12 | 24 | F | B | 1 | 1 |
| 13 | 25 | M | A | 0 | 1 |
| 14 | 38 | F | B | 1 | 1 |
| 15 | 38 | F | A | 1 | 0 |
| 16 | 43 | F | B | 1 | 0 |
| 17 | 43 | F | B | 1 | 0 |
| 18 | 45 | M | B | 1 | 0 |
| 19 | 37 | F | B | 1 | 0 |
| 20 | 43 | F | B | 1 | 0 |
| 21 | 36 | M | B | 1 | 0 |
| 22 | 42 | F | B | 1 | 1 |
| 23 | 22 | F | B | 1 | 1 |
| 24 | 47 | F | B | 1 | 0 |
| 25 | 36 | F | B | 1 | 0 |
| 26 | 50 | F | B | 2 | 0 |
| 27 | 47 | F | B | 1 | 1 |
| 28 | 47 | F | A | 1 | 1 |
| 29 | 44 | F | B | 1 | 0 |
| 30 | 44 | F | B | 1 | 1 |
| 31 | 38 | M | B | 1 | 1 |
| 32 | 48 | F | B | 1 | 1 |
| 33 | 49 | F | B | 0 | 0 |
| 34 | 47 | F | A | 0 | 1 |
| 35 | 45 | F | A | 0 | 1 |
| No. | Age (Year) | Sex | Tetany Test |
|---|---|---|---|
| 1 | 26 | F | 1 |
| 2 | 34 | M | 1 |
| 3 | 23 | F | 0 |
| 4 | 35 | F | 0 |
| 5 | 36 | M | 1 |
| 6 | 31 | F | 0 |
| 7 | 24 | F | 0 |
| 8 | 25 | M | 0 |
| 9 | 23 | F | 0 |
| 10 | 27 | F | 0 |
| 11 | 31 | F | 1 |
| 12 | 54 | F | 1 |
| 13 | 30 | M | 0 |
| 14 | 38 | M | 0 |
| 15 | 42 | M | 1 |
| 16 | 63 | F | 0 |
| 17 | 40 | F | 0 |
| 18 | 50 | M | 0 |
| 19 | 61 | F | 1 |
| 20 | 54 | F | 1 |
| 21 | 43 | F | 1 |
| 22 | 61 | F | 0 |
| 23 | 49 | F | 1 |
| 24 | 44 | F | 1 |
| No. | Mouth Paresthesia | Hand Paresthesia | Foot Paresthesia | Hand Cramps | Foot Cramps | Laryngospasms | Fasciculations of the Eyelide | Calf Cramps | Fainting | All Symptoms | Cardiac Arrhythmia | Dizziness | Sleep Disturbance | Anxiety Attacks | Tetany Test |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 0 | ++ | ++ | 0 | ++ | 0 | + | ++ | 0 | 2 | 0 | 0 | + | 0 | 1 |
| 2 | 0 | 0 | + | 0 | + | 0 | + | 0 | 0 | 2 | +++ | ++ | 0 | + | 1 |
| 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 4 | 0 | ++ | 0 | 0 | 0 | 0 | + | + | 0 | 2 | + | + | ++ | 0 | 1 |
| 5 | 0 | 0 | 0 | + | 0 | 0 | ++ | 0 | 0 | 1 | + | + | +++ | 0 | 1 |
| 6 | 0 | 0 | 0 | 0 | 0 | 0 | ++ | 0 | 0 | 1 | ++ | 0 | ++ | 0 | 1 |
| 7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 8 | 0 | 0 | ++ | ++ | ++ | 0 | ++ | ++ | ++ | 2 | ++ | 0 | ++ | 0 | 1 |
| 9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 11 | 0 | 0 | 0 | 0 | 0 | 0 | ++ | 0 | 0 | 1 | ++ | ++ | ++ | ++ | 1 |
| 12 | 0 | ++ | ++ | 0 | ++ | 0 | ++ | ++ | 0 | 2 | + | ++ | 0 | + | 1 |
| 13 | 0 | + | 0 | 0 | 0 | 0 | + | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| 14 | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | 2 | 0 | 0 | ++ | 0 | 1 |
| 15 | 0 | 0 | + | 0 | 0 | + | + | + | 0 | 2 | + | + | 0 | 0 | 0 |
| 16 | 0 | 0 | 0 | 0 | 0 | 0 | + | + | + | 2 | + | + | ++ | 0 | 0 |
| 17 | 0 | + | 0 | 0 | 0 | ++ | +++ | ++ | + | 2 | ++ | ++ | + | ++ | 0 |
| 18 | 0 | 0 | 0 | 0 | 0 | ++ | +++ | ++ | 0 | 2 | + | ++ | 0 | 0 | 0 |
| 19 | 0 | +++ | +++ | 0 | 0 | 0 | ++ | ++ | 0 | 2 | 0 | + | + | + | 0 |
| 20 | +++ | ++++ | +++ | +++ | +++ | ++++ | +++ | + | ++++ | 2 | ++++ | ++++ | ++++ | ++++ | 0 |
| 21 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ++ | ++ | 0 | ++ | 0 |
| 22 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ++ | ++ | ++ | ++ | 1 |
| 23 | 0 | 0 | 0 | 0 | + | 0 | ++ | 0 | 0 | 1 | 0 | 0 | ++ | 0 | 1 |
| 24 | 0 | 0 | 0 | 0 | + | 0 | 0 | 0 | 0 | 1 | 0 | ++ | 0 | 0 | 0 |
| 25 | 0 | 0 | 0 | 0 | 0 | 0 | ++ | ++ | 0 | 1 | 0 | ++ | 0 | 0 | 0 |
| 26 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 27 | 0 | + | + | 0 | 0 | 0 | + | ++ | 0 | 2 | 0 | + | + | + | 1 |
| 28 | 0 | + | 0 | 0 | 0 | 0 | + | + | 0 | 2 | + | + | + | + | 1 |
| 29 | 0 | + | 0 | 0 | 0 | + | 0 | + | 0 | 2 | 0 | ++ | ++ | 0 | 0 |
| 30 | 0 | ++ | 0 | 0 | 0 | 0 | ++ | 0 | 0 | 1 | + | ++ | + | ++ | 1 |
| 31 | 0 | 0 | + | 0 | 0 | 0 | 0 | + | 0 | 1 | 0 | + | 0 | + | 1 |
| 32 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 33 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 34 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | + | 0 | 0 | 0 | 1 |
| 35 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cegielska, J.; Szmidt-Sałkowska, E.; Domitrz, W.; Gaweł, M.; Radziwoń-Zaleska, M.; Domitrz, I. Migraine and Its Association with Hyperactivity of Cell Membranes in the Course of Latent Magnesium Deficiency—Preliminary Study of the Importance of the Latent Tetany Presence in the Migraine Pathogenesis. Nutrients 2021, 13, 2701. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082701
Cegielska J, Szmidt-Sałkowska E, Domitrz W, Gaweł M, Radziwoń-Zaleska M, Domitrz I. Migraine and Its Association with Hyperactivity of Cell Membranes in the Course of Latent Magnesium Deficiency—Preliminary Study of the Importance of the Latent Tetany Presence in the Migraine Pathogenesis. Nutrients. 2021; 13(8):2701. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082701
Chicago/Turabian StyleCegielska, Joanna, Elżbieta Szmidt-Sałkowska, Wojciech Domitrz, Małgorzata Gaweł, Maria Radziwoń-Zaleska, and Izabela Domitrz. 2021. "Migraine and Its Association with Hyperactivity of Cell Membranes in the Course of Latent Magnesium Deficiency—Preliminary Study of the Importance of the Latent Tetany Presence in the Migraine Pathogenesis" Nutrients 13, no. 8: 2701. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082701