
Vitamin D Status and Gestational Diabetes in Russian Pregnant Women in the Period between 2012 and 2021: A Nested Case–Control Study

 ,
,  , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- The prospective observational study of early markers of GDM conducted from January 2012 to December 2014;
- GEM-GDM randomized controlled trial (Genetic and Epigenetic Mechanisms of Developing Gestational Diabetes Mellitus and Its Effects on the Fetus) performed from July 2015 to July 2021 [35].
2.2. Assessment of Biochemical Parameters
2.3. Statistical Analysis
3. Results
3.1. Characteristics and Vitamin D Status of Women with and without GDM
3.2. Vitamin D Status in the Third Trimester and Related Characteristics of Pregnant Women Participating in the Period 2012–2014 and 2018–2021
3.3. 25OH-Vitamin D Levels Change during Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021; Available online: https://www.diabetesatlas.org (accessed on 29 March 2022).
- HAPO Study Cooperative Research Group; Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R. Hyperglycemia and Adverse Pregnancy Outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Haroush, A.; Yogev, Y.; Hod, M. Epidemiology of Gestational Diabetes Mellitus and Its Association with Type 2 Diabetes. Diabet. Med. 2004, 21, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Giannakou, K.; Evangelou, E.; Yiallouros, P.; Christophi, C.A.; Middleton, N.; Papatheodorou, E.; Papatheodorou, S.I. Risk Factors for Gestational Diabetes: An Umbrella Review of Meta-Analyses of Observational Studies. PLoS ONE 2019, 14, e0215372. [Google Scholar] [CrossRef] [PubMed]
- Popova, P.V.; Grineva, E.N.; Gerasimov, A.S.; Kravchuk, E.N.; Ryazantseva, E.M.; Shelepova, E.S. The New Combination of Risk Factors Determining a High Risk of Gestational Diabetes Mellitus. Minerva Endocrinol. 2015, 40, 239–247. [Google Scholar]
- Plows, J.; Stanley, J.; Baker, P.; Reynolds, C.; Vickers, M. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [Green Version]
- Burris, H.H.; Camargo, C.A. Vitamin D and Gestational Diabetes Mellitus. Curr. Diab. Rep. 2014, 14, 451. [Google Scholar] [CrossRef] [Green Version]
- Clifton-Bligh, R.J.; McElduff, P.; McElduff, A. Maternal Vitamin D Deficiency, Ethnicity and Gestational Diabetes. Diabet. Med. 2008, 25, 678–684. [Google Scholar] [CrossRef]
- Hossein-Nezhad, A.; Maghbooli, Z.; Vassigh, A.-R.; Larijani, B. Prevalence of Gestational Diabetes Mellitus and Pregnancy Outcomes in Iranian Women. Taiwan J. Obstet. Gynecol. 2007, 46, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Qiu, C.; Hu, F.B.; David, R.M.; van Dam, R.M.; Bralley, A.; Williams, M.A. Maternal Plasma 25-Hydroxyvitamin D Concentrations and the Risk for Gestational Diabetes Mellitus. PLoS ONE 2008, 3, e3753. [Google Scholar] [CrossRef] [Green Version]
- Farrant, H.J.W.; Krishnaveni, G.V.; Hill, J.C.; Boucher, B.J.; Fisher, D.J.; Noonan, K.; Osmond, C.; Veena, S.R.; Fall, C.H.D. Vitamin D Insufficiency Is Common in Indian Mothers but Is Not Associated with Gestational Diabetes or Variation in Newborn Size. Eur. J. Clin. Nutr. 2009, 63, 646–652. [Google Scholar] [CrossRef] [Green Version]
- Makgoba, M.; Nelson, S.M.; Savvidou, M.; Messow, C.-M.; Nicolaides, K.; Sattar, N. First-Trimester Circulating 25-Hydroxyvitamin D Levels and Development of Gestational Diabetes Mellitus. Diabetes Care 2011, 34, 1091–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griew, K.; Nunn, R.; Fairbrother, G.; Tewari, S. Early Pregnancy Vitamin D Deficiency and Gestational Diabetes: Exploring the Link. Aust. J. Gen. Pract. 2019, 48, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.-H.; Kung, W.-J.; Lee, C.-H.; Zen, Y.-H.; Lee, C.-F.; Yang, H.-R.; Lin, C.-C.; Huang, Y.-L. High Levels of 25-OH-Vitamin D and Copper in Pregnant Women with Abnormal Glucose Challenge Test. Biol. Trace Elem. Res. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Amraei, M.; Mohamadpour, S.; Sayehmiri, K.; Mousavi, S.F.; Shirzadpour, E.; Moayeri, A. Effects of Vitamin D Deficiency on Incidence Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2018, 9, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.; Zhang, Y.; Wang, X.; You, L.; Xu, P.; Cui, X.; Zhu, L.; Ji, C.; Guo, X.; Wen, J. Maternal Vitamin D Status and Risk of Gestational Diabetes: A Meta-Analysis. Cell Physiol. Biochem. 2018, 45, 291–300. [Google Scholar] [CrossRef]
- Milajerdi, A.; Abbasi, F.; Mousavi, S.M.; Esmaillzadeh, A. Maternal Vitamin D Status and Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Clin. Nutr. 2021, 40, 2576–2586. [Google Scholar] [CrossRef]
- Zhang, M.-X.; Pan, G.-T.; Guo, J.-F.; Li, B.-Y.; Qin, L.-Q.; Zhang, Z.-L. Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients 2015, 7, 8366–8375. [Google Scholar] [CrossRef] [Green Version]
- Lu, M.; Xu, Y.; Lv, L.; Zhang, M. Association between Vitamin D Status and the Risk of Gestational Diabetes Mellitus: A Meta-Analysis. Arch. Gynecol. Obstet. 2016, 293, 959–966. [Google Scholar] [CrossRef]
- Popova, P.; Castorino, K.; Grineva, E.; Kerr, D. Gestational Diabetes Mellitus Diagnosis and Treatment Goals: Measurement and Measures. Minerva Endocrinol. 2016, 41, 421–432. [Google Scholar]
- Rizzo, G.; Garzon, S.; Fichera, M.; Panella, M.M.; Catena, U.; Schiattarella, A.; de Franciscis, P.; Vilos, G.; Tesarik, J.; Török, P.; et al. Vitamin D and Gestational Diabetes Mellitus: Is There a Link? Antioxidants 2019, 8, 511. [Google Scholar] [CrossRef] [Green Version]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of Vitamin D Supplementation during Pregnancy on Maternal and Neonatal Outcomes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Fertil. Steril. 2015, 103, 1278–1288.e4. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; De-Regil, L.M.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D Supplementation during Pregnancy: Updated Meta-Analysis on Maternal Outcomes. J. Steroid Biochem. Mol. Biol. 2016, 164, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios, C.; Kostiuk, L.K.; Peña-Rosas, J.P. Vitamin D Supplementation for Women during Pregnancy. Cochrane Database Syst. Rev. 2019, 7, CD008873. [Google Scholar] [CrossRef] [PubMed]
- Griffith, R.J.; Alsweiler, J.; Moore, A.E.; Brown, S.; Middleton, P.; Shepherd, E.; Crowther, C.A. Interventions to Prevent Women from Developing Gestational Diabetes Mellitus: An Overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2020, 6, CD012394. [Google Scholar] [CrossRef]
- Ojo, O.; Weldon, S.M.; Thompson, T.; Vargo, E.J. The Effect of Vitamin D Supplementation on Glycaemic Control in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 1716. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association Professional Practice Committee. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S232–S243. [Google Scholar] [CrossRef]
- Committee on Practice Bulletins–Obstetrics. Practice bulletin No. 137: Gestational diabetes mellitus. Obstet. Gynecol. 2013, 122, 406–416. [Google Scholar] [CrossRef]
- Dedov, I.I.; Krasnopol’skiy, V.I.; Sukhikh, G.T. Russian National Consensus Statement on gestational diabetes: Diagnostics, treatment and postnatal care. Diabetes Mellit. 2012, 15, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Guardo, F.D.; Currò, J.M.; Valenti, G.; Rossetti, P.; Di Gregorio, L.M.; Conway, F.; Chiofalo, B.; Garzon, S.; Bruni, S.; Rizzo, G. Non-pharmacological management of gestational diabetes: The role of myo-inositol. J. Complement. Integr. Med. 2019, 17, 17. [Google Scholar] [CrossRef]
- Fichera, M.; Török, P.; Tesarik, J.; Della Corte, L.; Rizzo, G.; Garzon, S.; Carlea, A.; Di Angelo, A.S.; Zito, G.; Panella, M.M. Vitamin D, reproductive disorders and assisted reproduction: Evidences and perspectives. Int. J. Food Sci. Nutr. 2020, 71, 276–285. [Google Scholar] [CrossRef]
- Gorelova, I.V.; Popova, P.V.; Rulev, M.V. Vitamin D and Reproductive Health. Probl. Endocrinol. 2020, 66, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pigarova, E.A.; Rozhinskaya, L.Y.; Belaya, J.E.; Dzeranova, L.K.; Karonova, T.L.; Ilyin, A.V.; Melnichenko, G.A.; Dedov, I.I. Russian Association of Endocrinologists Recommendations for Diagnosis, Treatment and Prevention of Vitamin D Deficiency in Adults. Probl. Endocrinol. 2016, 62, 60–84. [Google Scholar] [CrossRef]
- Popova, P.; Vasilyeva, L.; Tkachuck, A.; Puzanov, M.; Golovkin, A.; Bolotko, Y.; Pustozerov, E.; Vasilyeva, E.; Li, O.; Zazerskaya, I.; et al. A Randomised, Controlled Study of Different Glycaemic Targets during Gestational Diabetes Treatment: Effect on the Level of Adipokines in Cord Blood and ANGPTL4 Expression in Human Umbilical Vein Endothelial Cells. Int. J. Endocrinol. 2018, 2018, 6481658. [Google Scholar] [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Etminan-Baksh, M.; Tadi, S.; Hatami, M.; Darabi, R. Prevalence of Gestational Diabetes Mellitus and Its Associated Risk Factors in Boo-Ali Hospital, Tehran. Galen Med. J. 2020, 9, e1642. [Google Scholar] [CrossRef]
- St. Luke’s Medical Center, Quezon City, Philippines; Cabrera, C.C.; Dampil, O.A.; Ong-Lopez, A.M. The Association between Maternal Serum Vitamin D Levels and Gestational Diabetes Mellitus among Filipino Patients: A Cross-Sectional Study. J. ASEAN Fed. Endocr. Soc. 2020, 35, 169–175. [Google Scholar] [CrossRef]
- Zhu, B.; Huang, K.; Yan, S.; Hao, J.; Zhu, P.; Chen, Y.; Ye, A.; Tao, F. VDR Variants Rather than Early Pregnancy Vitamin D Concentrations Are Associated with the Risk of Gestational Diabetes: The Ma’anshan Birth Cohort (MABC) Study. J. Diabetes Res. 2019, 2019, 8313901. [Google Scholar] [CrossRef]
- Pham, T.T.M.; Huang, Y.-L.; Chao, J.C.-J.; Chang, J.-S.; Chen, Y.-C.; Wang, F.-F.; Bai, C.-H. Plasma 25(OH)D Concentrations and Gestational Diabetes Mellitus among Pregnant Women in Taiwan. Nutrients 2021, 13, 2538. [Google Scholar] [CrossRef]
- Corcoy, R.; Mendoza, L.C.; Simmons, D.; Desoye, G.; Adelantado, J.M.; Chico, A.; Devlieger, R.; van Assche, A.; Galjaard, S.; Timmerman, D.; et al. The DALI Vitamin D Randomized Controlled Trial for Gestational Diabetes Mellitus Prevention: No Major Benefit Shown besides Vitamin D Sufficiency. Clin. Nutr. 2020, 39, 976–984. [Google Scholar] [CrossRef] [Green Version]
- Harreiter, J.; Desoye, G.; van Poppel, M.N.M.; Kautzky-Willer, A.; Dunne, F.; Corcoy, R.; Devlieger, R.; Simmons, D.; Adelantado, J.M.; Damm, P.; et al. The Effects of Lifestyle and/or Vitamin D Supplementation Interventions on Pregnancy Outcomes: What Have We Learned from the DALI Studies? Curr. Diab. Rep. 2019, 19, 162. [Google Scholar] [CrossRef] [PubMed]
- Nausheen, S.; Habib, A.; Bhura, M.; Rizvi, A.; Shaheen, F.; Begum, K.; Iqbal, J.; Ariff, S.; Shaikh, L.; Raza, S.S.; et al. Impact Evaluation of the Efficacy of Different Doses of Vitamin D Supplementation during Pregnancy on Pregnancy and Birth Outcomes: A Randomised, Controlled, Dose Comparison Trial in Pakistan. BMJ Nutr. Prev. Health 2021, 4, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Karonova, T.; Andreeva, A.; Nikitina, I.; Belyaeva, O.; Mokhova, E.; Galkina, O.; Vasilyeva, E.; Grineva, E. Prevalence of Vitamin D Deficiency in the North-West Region of Russia: A Cross-Sectional Study. J. Steroid Biochem. Mol. Biol. 2016, 164, 230–234. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Women with GDM N = 138 | Women without GDM N = 180 | p | |
|---|---|---|---|
| Age | 31 [28.0–34.0] | 29 [26.0–33.0] | 0.005 |
| Pre-gestational BMI | 23.4 [21.4–27.2] | 22.4 [20.4–24.9] | 0.010 |
| Family history of diabetes, N (%) | 56 (40.0) | 63 (34.2) | 0.287 |
| History of arterial hypertension, N (%) | 19 (13.6) | 12 (6.5) | 0.033 |
| History of GDM, N (%) | 6 (7.2) | 2 (2.0) | 0.144 |
| History of IGT, N (%) | 3 (2.1) | 3 (1.6) | 1.000 |
| PCOS, N (%) | 8 (5.7) | 11 (6.0) | 0.911 |
| Parity: | |||
| Nulliparae, N (%) | 91 (65.0) | 111 (60.3) | 0.390 |
| Multiparae, N (%) | 49 (35.0) | 73 (39.7) | |
| Fasting plasma glucose (mmol/L) | 5.2 [4.7–5.4] | 4.3 [4.0–4.5] | <0.001 |
| 1 h postload glucose (mmol/L) | 9.0 [7.6–10.1] | 6.7 [5.7–7.6] | <0.001 |
| 2 h postload glucose (mmol/L) | 7.6 [6.0–8.8] | 6.0 [5.1–6.5] | <0.001 |
| Vitamin D supplements intake in the first trimester, N (%) | 37 (29.1) | 34 (21.2) | 0.124 |
| Vitamin D supplements intake during pregnancy, N (%) | |||
| No | 30 (23.6) | 53 (33.1) | 0.134 |
| <1 month | 28 (22.0) | 42 (26.2) | |
| 1–3 months | 27 (21.3) | 25 (15.6) | |
| >3 months | 42 (33.1) | 40 (25.0) | |
| Doses of cholecalciferol, IU *** | 400 [400–2400] | 400 [400–400] | <0.001 |
| Gestational age at the time of 25(OH)D analysis in the 1st trimester, weeks * | 11 [8–13] | 10 [8–12] | 0.028 |
| First trimester 25(OH)D level, ng/mL * | 20.0 [15.1–25.7] | 20.5 [14.4–27.5] | 0.565 |
| Severe vitamin D deficiency in the first trimester (<10 ng/mL), N (%) * | 5 (6.0) | 3 (2.3) | 0.266 |
| Vitamin D deficiency in the first trimester (>10 and <20 ng/mL), N (%) * | 36 (43.4) | 57 (43.5) | 0.608 |
| Vitamin D insufficiency in the first trimester (>20 and <30 ng/mL), N (%) * | 32 (38.6) | 46 (35.1) | 0.610 |
| Adequate level of 25(OH)D in the first trimester, N (%) * | 10 (12.0) | 25 (19.1) | 0.175 |
| Excessive level of 25(OH)D in the first trimester (>100 ng/mL) | 0 | 0 | |
| Gestational age at the time of 25(OH)D analysis in the 3rd trimester, weeks ** | 26.5 [25.0–29.0] | 26.0 [25.0–28.2] | 0.438 |
| Third trimester 25(OH)D level, ng/mL ** | 25.3 [19.7–32.9] | 26.7 [20.7–36.7] | 0.471 |
| Severe vitamin D deficiency in the third trimester (<10 ng/mL), N (%) | 2 (1.9) | 6 (6.3) | 0.151 |
| Vitamin D deficiency in the third trimester (>10 and <20 ng/mL), N (%) | 26 (24.3) | 15 (15.8) | 0.133 |
| Vitamin D insufficiency in the third trimester (>20 and <30 ng/mL), N (%) | 42 (39.2) | 40 (42.1) | 0.680 |
| Adequate level of 25(OH)D in the third trimester, N (%) | 37 (34.6) | 34 (35.8) | 0.857 |
| Excessive level of 25(OH)D in the third trimester (>100 ng/mL) | 0 | 0 |
| Vitamin D Levels | Crude Model | Adjusted Model * | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| First trimester 25(OH)D concentration | 0.98 | 0.95–1.02 | 0.315 | 1.03 | 0.95–1.06 | 0.244 |
| First-trimester vitamin D insufficiency | ||||||
| ≥30 ng/mL | 1.00 | 0.168 | 1.00 | 0.222 | ||
| <30 ng/mL | 1.72 | 0.78–3.80 | 1.39 | 0.38–5.07 | ||
| First-trimester vitamin D deficiency | ||||||
| ≥20 ng/mL | 1.00 | 0.608 | 1.00 | 0.218 | ||
| <20 ng/mL | 1.16 | 0.67–2.00 | 1.32 | 0.48–3.61 | ||
| Third trimester 25(OH)D concentration | 0.99 | 0.97–1.01 | 0.443 | 1.00 | 0.96–1.03 | 0.486 |
| Third-trimester vitamin D insufficiency | ||||||
| ≥30 ng/mL | 1.00 | 0.857 | 1.00 | 0.489 | ||
| <30 ng/mL | 1.05 | 0.59–1.88 | 1.17 | 0.50–2.41 | ||
| Third-trimester vitamin D deficiency | ||||||
| ≥20 ng/mL | 1.00 | 0.501 | 1.00 | 0.494 | ||
| <20 ng/mL | 1.25 | 0.65–2.39 | 1.08 | 0.44–2.66 | ||
| Women Participating in 2012–2014 N = 98 * | Women Participating in 2018–2021 N = 104 * | p | |
|---|---|---|---|
| Age | 30 [27–33] | 31 [28–35] | 0.008 |
| Pre-gestational BMI | 23.3 [20.9–26.9] | 22.2 [20.4–24.8] | 0.098 |
| N (%) of women with GDM | 51 (52.0%) | 56 (53.8%) | 0.888 |
| Family history of diabetes, N (%) | 40 (40.8) | 40 (38.5) | 0.732 |
| History of arterial hypertension, N (%) | 10 (10.2) | 5 (4.8) | 0.183 |
| History of GDM, N (%) | 1 (1.0) | 6 (5.8) | 1.000 |
| History of IGT, N (%) | 4 (4.1) | 0 (0.0) | 0.054 |
| PCOS, N (%) | 4 (4.1) | 7 (6.7) | 0.539 |
| Parity: | |||
| Nulliparae, N (%) | 70 (71.4) | 62 (59.6) | 0.078 |
| Multiparae, N (%) | 28 (28.6) | 42 (40.4) | |
| Fasting plasma glucose (mmol/L) | 4.7 [4.4–5.3] | 4.6 [4.2–5.1] | 0.072 |
| 1 h postload glucose (mmol/L) | 7.8 ± 1.9 | 7.7 ± 1.7 | 0.457 |
| 2 h postload glucose (mmol/L) | 6.4 [5.5–8.2] | 6.5 [5.5–7.7] | 0.777 |
| Vitamin D supplements intake in the first trimester, N (%) | 21 (23.1) | 28 (29.8) | 0.301 |
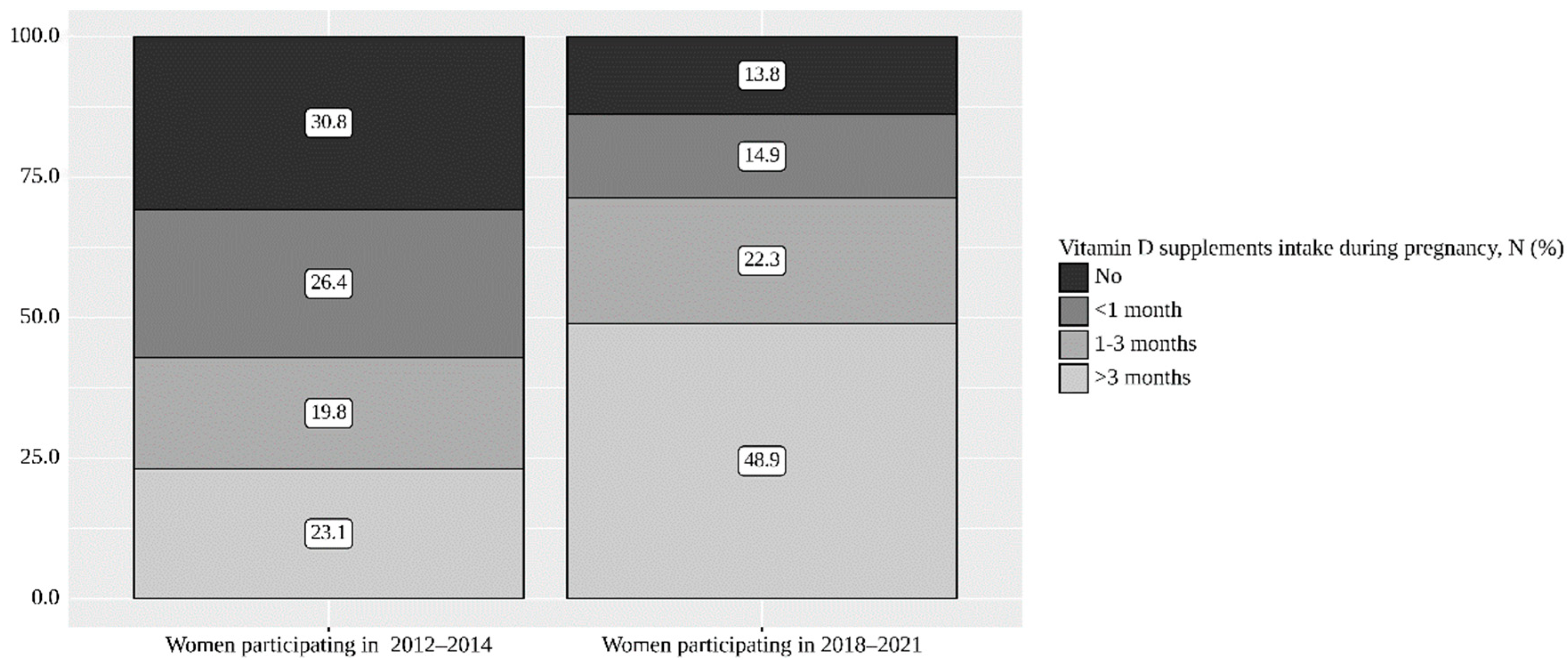
| Vitamin D supplements intake during pregnancy, N (%) | |||
| No | 28 (30.8%) | 13 (13.8%) | <0.001 |
| <1 month | 24 (26.4%) | 14 (14.9%) | |
| 1–3 months | 18 (19.8%) | 21 (22.3%) | |
| >3 months | 21 (23.1%) | 46 (48.9%) | |
| Doses of cholecalciferol, ME ** | - | 400 [400–2000] | - |
| Third trimester 25(OH)D level, ng/mL | 25.6 [20.0–32.8] | 26.3 [20.3–35.0] | 0.827 |
| Severe vitamin D deficiency in the third trimester (<10 ng/mL), N (%) | 3 (3.1) | 5 (4.8) | 0.722 |
| Vitamin D deficiency in the third trimester (>10 and <20 ng/mL), N (%) | 22 (22.4) | 19 (18.3) | 0.460 |
| Vitamin D insufficiency in the third trimester (>20 and <30 ng/mL), N (%) | 39 (39.8) | 43 (41.3) | 0.823 |
| Adequate level of 25(OH)D, N (%) | 34 (34.7) | 37 (35.6) | 0.895 |
| Excessive (>100 ng/mL) | 0 | 0 |
| Serum 25(OH)D Levels, Me [Q1–Q3], ng/mL | p | ||
|---|---|---|---|
| 1st Trimester | 3rd Trimester | ||
| Women with GDM, N= 49 | 19.1 [14.0–26.5] | 25.2 [19.3–32.3] | <0.001 |
| Women without GDM, N = 42 | 22.8 [13.5–30.2] | 26.8 [21.5–35.1] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tkachuk, A.S.; Vasukova, E.A.; Anopova, A.D.; Karonova, T.L.; Pustozerov, E.A.; Teplova, Y.A.; Eriskovskaya, A.I.; Isakov, A.O.; Vasilieva, E.Y.; Kokina, M.A.; et al. Vitamin D Status and Gestational Diabetes in Russian Pregnant Women in the Period between 2012 and 2021: A Nested Case–Control Study. Nutrients 2022, 14, 2157. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102157
Tkachuk AS, Vasukova EA, Anopova AD, Karonova TL, Pustozerov EA, Teplova YA, Eriskovskaya AI, Isakov AO, Vasilieva EY, Kokina MA, et al. Vitamin D Status and Gestational Diabetes in Russian Pregnant Women in the Period between 2012 and 2021: A Nested Case–Control Study. Nutrients. 2022; 14(10):2157. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102157
Chicago/Turabian StyleTkachuk, Aleksandra S., Elena A. Vasukova, Anna D. Anopova, Tatiana L. Karonova, Evgenii A. Pustozerov, Yana A. Teplova, Angelina I. Eriskovskaya, Artem O. Isakov, Elena Y. Vasilieva, Maria A. Kokina, and et al. 2022. "Vitamin D Status and Gestational Diabetes in Russian Pregnant Women in the Period between 2012 and 2021: A Nested Case–Control Study" Nutrients 14, no. 10: 2157. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102157