Poor Sleep Quality Decreases Concurrent Training Benefits in Markers of Metabolic Syndrome and Quality of Life of Morbidly Obese Patients

 ,
, 
 ,
, 
 ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
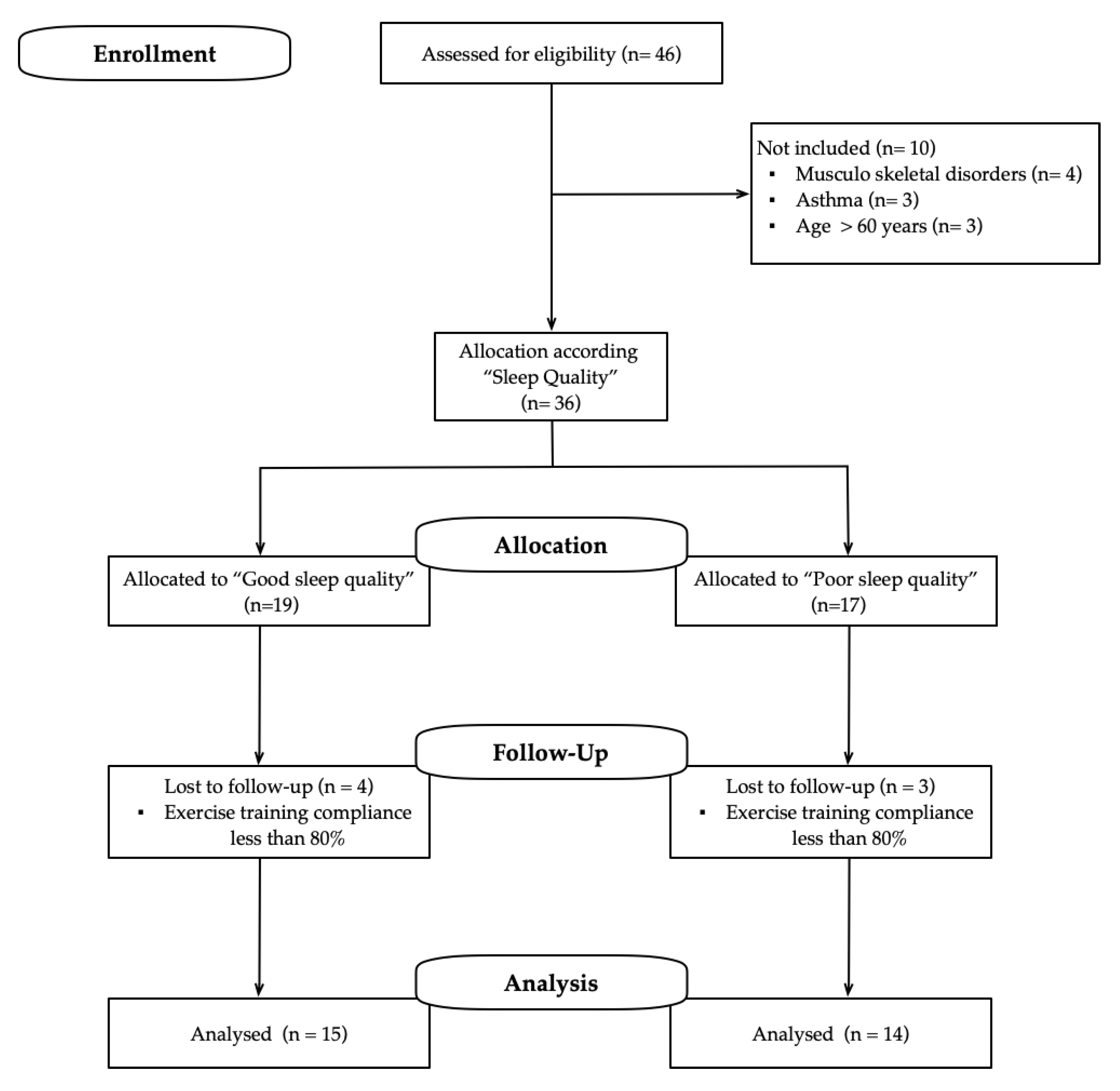
2.1. Study Design
2.2. Patients and Recruitment
2.3. Measurements
2.3.1. SQ Measurements
2.3.2. MetS Markers
2.3.3. HRQoL
2.3.4. Body Composition and Anthropometrics Parameters
2.4. CT Intervention
2.5. Data Analysis
3. Results
3.1. Baseline Characteristics
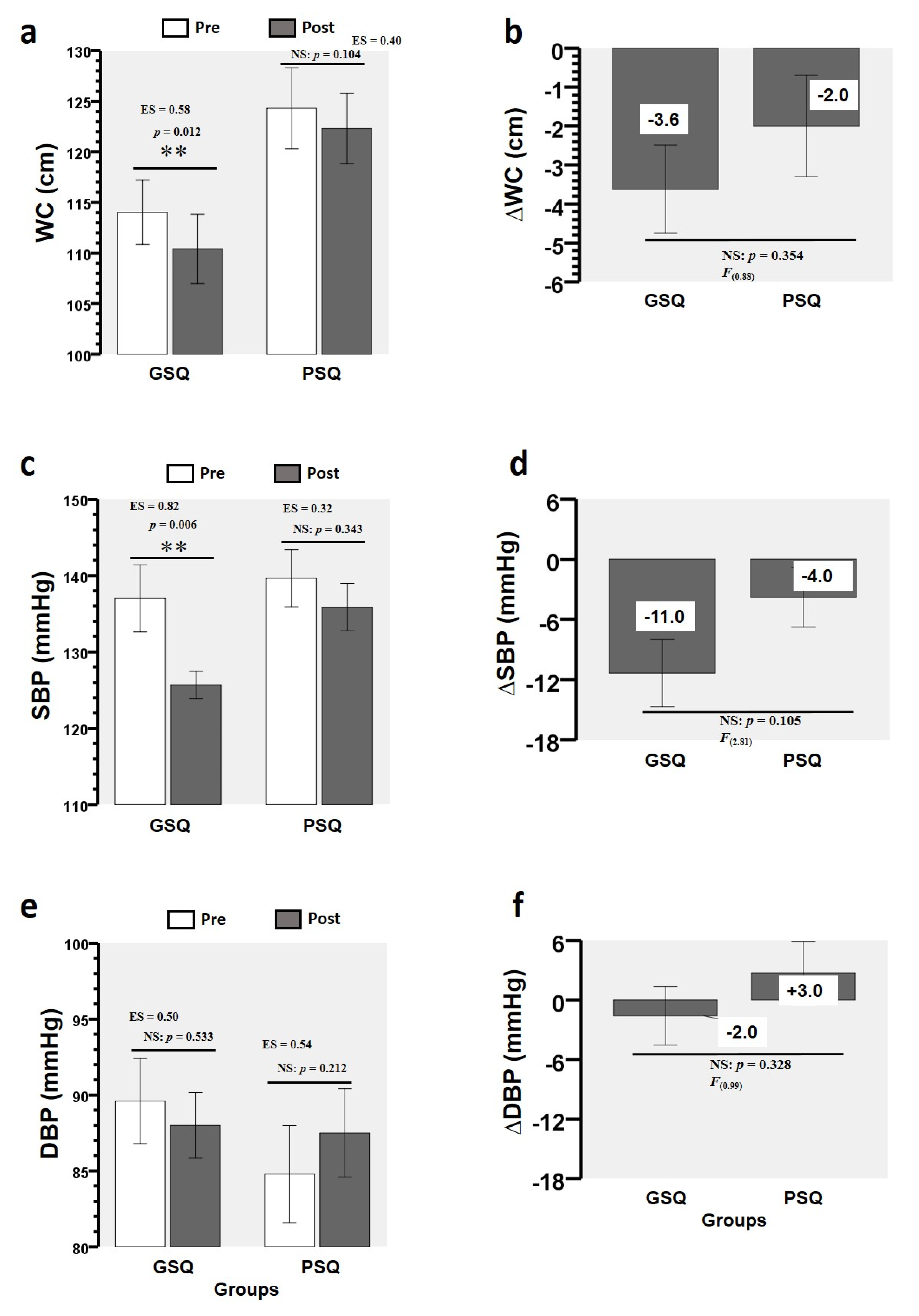
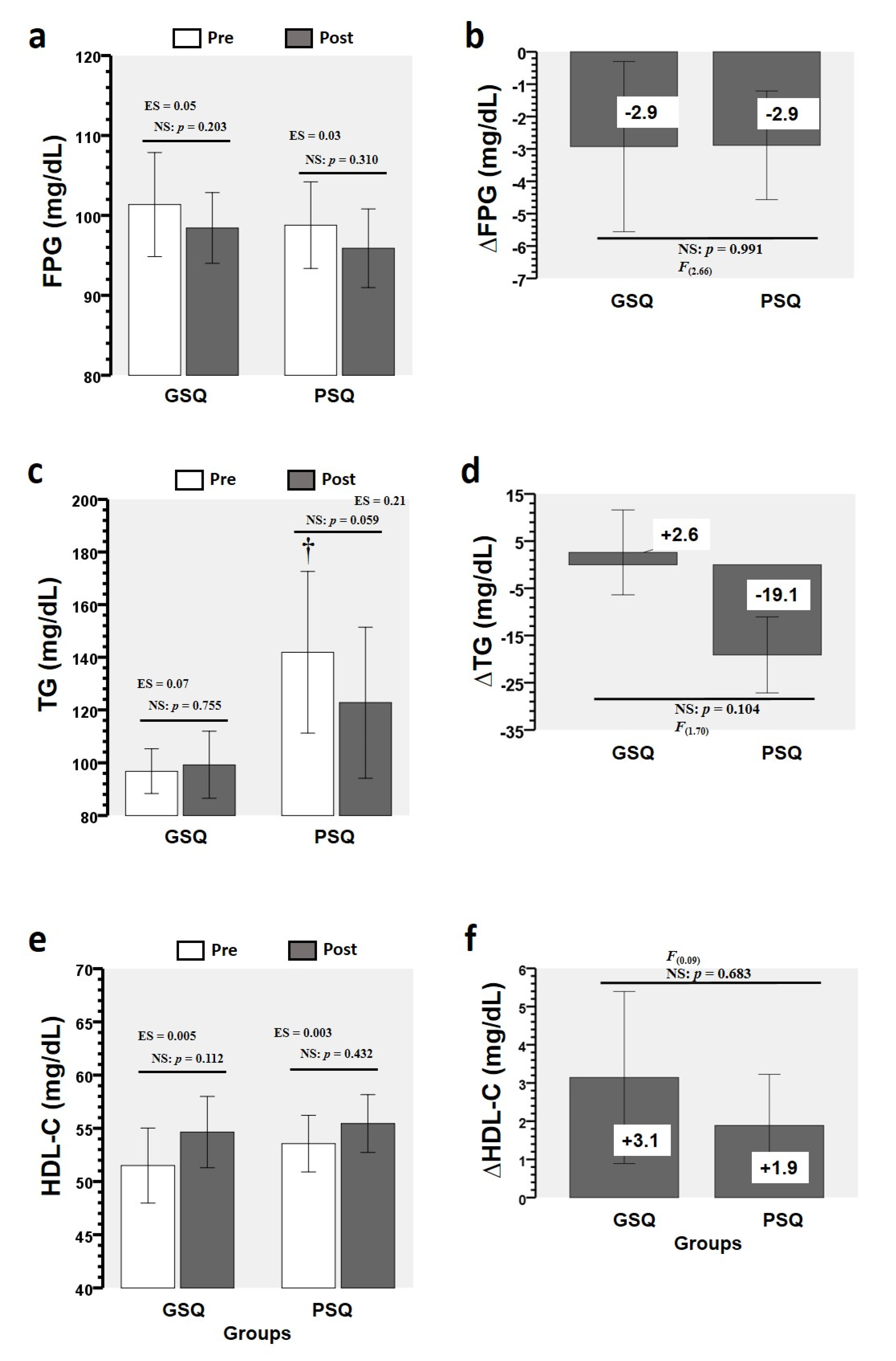
3.2. Training-Induced Changes in MetS Markers
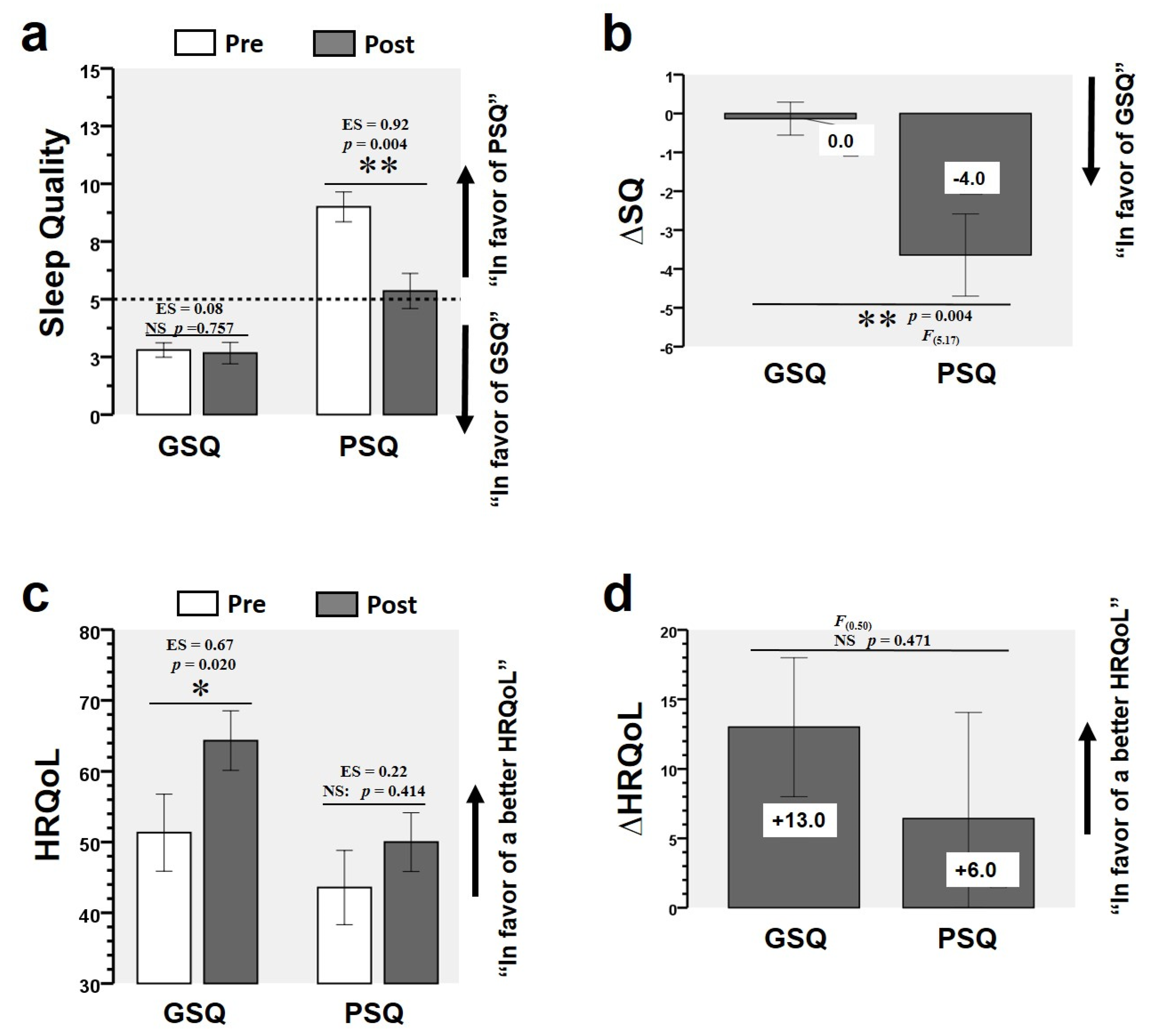
3.3. Training-Induced Changes in SQ and HRQoL
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baffi, C.W.; Wood, L.; Winnica, D.; Strollo, P.J., Jr.; Gladwin, M.T.; Que, L.G.; Holguin, F. Metabolic Syndrome and the Lung. Chest 2016, 149, 1525–1534. [Google Scholar] [CrossRef] [Green Version]
- Duval, K.; Marceau, P.; Lescelleur, O.; Hould, F.S.; Marceau, S.; Biron, S.; Lebel, S.; Perusse, L.; Lacasse, Y. Health-related quality of life in morbid obesity. Obes. Surg. 2006, 16, 574–579. [Google Scholar] [CrossRef]
- Raveendran, R.; Wong, J.; Chung, F. Morbid obesity, sleep apnea, obesity hypoventilation syndrome: Are we sleepwalking into disaster? Perioper. Care Oper. Room Manag. 2017, 9, 24–32. [Google Scholar] [CrossRef]
- Araghi, M.H.; Jagielski, A.; Neira, I.; Brown, A.; Higgs, S.; Thomas, G.N.; Taheri, S. The complex associations among sleep quality, anxiety-depression, and quality of life in patients with extreme obesity. Sleep 2013, 36, 1859–1865. [Google Scholar] [CrossRef] [Green Version]
- Beccuti, G.; Pannain, S. Sleep and obesity. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Hargens, T.A.; Kaleth, A.S.; Edwards, E.S.; Butner, K.L. Association between sleep disorders, obesity, and exercise: A review. Nat. Sci. Sleep 2013, 5, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K.; Saltin, B. Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [Green Version]
- Boutcher, S.; Dunn, S.L. Factors that may impede the weight loss response to exercise-based interventions. Obes. Rev. 2009, 10, 671–680. [Google Scholar] [CrossRef]
- Tjønna, A.E.; Ramos, J.S.; Pressler, A.; Halle, M.; Jungbluth, K.; Ermacora, E.; Salvesen, Ø.; Rodrigues, J.; Bueno, C.R.; Munk, P.S. EX-MET study: Exercise in prevention on of metabolic syndrome–a randomized multicenter trial: Rational and design. BMC Public Health 2018, 18, 437. [Google Scholar] [CrossRef]
- Ostman, C.; Smart, N.A.; Morcos, D.; Duller, A.; Ridley, W.; Jewiss, D. The effect of exercise training on clinical outcomes in patients with the metabolic syndrome: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2017, 16, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardinal, B.J.; Park, E.A.; Kim, M.; Cardinal, M.K. If exercise is medicine, where is exercise in medicine? Review of US medical education curricula for physical activity-related content. J. Phys. Act. Health 2015, 12, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Ratamess, N.A. Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 674–688. [Google Scholar] [CrossRef] [PubMed]
- Huck, C.J. Effects of supervised resistance training on fitness and functional strength in patients succeeding bariatric surgery. J. Strength Cond. Res. 2015, 29, 589–595. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Correa-Rodríguez, M.; Tordecilla-Sanders, A.; Aya-Aldana, V.; Izquierdo, M.; Correa-Bautista, J.E.; Álvarez, C.; Garcia-Hermoso, A. Exercise and postprandial lipemia: Effects on vascular health in inactive adults. Lipids Health Dis. 2018, 17, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramírez-Vélez, R.; Hernández-Quiñones, P.A.; Tordecilla-Sanders, A.; Álvarez, C.; Ramírez-Campillo, R.; Izquierdo, M.; Correa-Bautista, J.E.; Garcia-Hermoso, A.; Garcia, R.G. Effectiveness of HIIT compared to moderate continuous training in improving vascular parameters in inactive adults. Lipids Health Dis. 2019, 18, 42. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, C.; Ramírez-Campillo, R.; Cristi-Montero, C.; Ramírez-Vélez, R.; Izquierdo, M. Prevalence of Non-responders for Blood Pressure and Cardiometabolic Risk Factors Among Prehypertensive Women After Long-Term High-Intensity Interval Training. Front. Physiol. 2018, 9, 1443. [Google Scholar] [CrossRef] [Green Version]
- Pescatello, L.S.; MacDonald, H.V.; Lamberti, L.; Johnson, B.T. Exercise for hypertension: A prescription update integrating existing recommendations with emerging research. Curr. Hypertens. Rep. 2015, 17, 87. [Google Scholar] [CrossRef] [Green Version]
- Lemes, I.R.; Ferreira, P.H.; Linares, S.N.; Machado, A.F.; Pastre, C.M.; Netto, J.J. Resistance training reduces systolic blood pressure in metabolic syndrome: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1438–1442. [Google Scholar] [CrossRef]
- Spiegel, K.; Tasali, E.; Penev, P.; Van Cauter, E. Brief communication: Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, B.; Fernandes, S.; Davis, F. Science of sleep and sports performance–a scoping review. Sci. Sports 2020, 35, 3–11. [Google Scholar] [CrossRef]
- Delgado-Floody, P.; Álvarez, C.; Lusa-Cadore, E.; Flores-Opazo, M.; Caamaño-Navarrete, F.; Izquierdo, M. Preventing Metabolic Syndrome in Morbid Obesity With Resistance Training: Reporting Interindividual Variability. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1368–1381. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Rahe, C.; Czira, M.E.; Teismann, H.; Berger, K. Associations between poor sleep quality and different measures of obesity. Sleep Med. 2015, 16, 1225–1228. [Google Scholar] [CrossRef]
- Toor, P.; Kim, K.; Buffington, C.K. Sleep quality and duration before and after bariatric surgery. Obes. Surg. 2012, 22, 890–895. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T.; et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [Green Version]
- North American Association for the Study of Obesity; National Heart; Lung, Blood Institute; NHLBI Obesity Education Initiative. The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults; The Institute: Washington, DC, USA, 2000. [Google Scholar]
- Ware, J.E. SF-36 Health Survey: SF-36 Health Survey Manual and Interpretation Guide; Health Assessment Lab: Boston, MA, USA, 2000. [Google Scholar]
- Sturm, R. Increases in morbid obesity in the USA: 2000–2005. Public Health 2007, 121, 492–496. [Google Scholar] [CrossRef] [Green Version]
- Brzycki, M. Strength testing—Predicting a one-rep max from reps-to-fatigue. J. Phys. Educ. Recreat. Dance 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Calhoun, D.A.; Harding, S.M. Sleep and hypertension. Chest 2010, 138, 434–443. [Google Scholar] [CrossRef]
- Picó-Sirvent, I.; Aracil-Marco, A.; Pastor, D.; Moya-Ramón, M. Effects of a Combined High-Intensity Interval Training and Resistance Training Program in Patients Awaiting Bariatric Surgery: A Pilot Study. Sports 2019, 7, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, M.; Goldsworthy, U.R.; Cary, B.A.; Hill, C.J. A diet and exercise program to improve clinical outcomes in patients with obstructive sleep apnea—A feasibility study. J. Clin. Sleep Med. 2009, 5, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Floody, P.; Caamaño-Navarrete, F.; Jerez-Mayorga, D.; Martínez-Salazar, C.; García-Pinillos, F.; Latorre-Román, P. Adaptaciones al ejercicio físico en el perfil lipídico y la salud cardiovascular de obesos mórbidos. Gac. Med. Mex. 2017, 153, 781–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroeder, E.C.; Franke, W.D.; Sharp, R.L.; Lee, D.C. Comparative effectiveness of aerobic, resistance, and combined training on cardiovascular disease risk factors: A randomized controlled trial. PLoS ONE 2019, 14, e0210292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendelson, M.; Borowik, A.; Michallet, A.S.; Perrin, C.; Monneret, D.; Faure, P.; Levy, P.; Pepin, J.L.; Wuyam, B.; Flore, P. Sleep quality, sleep duration and physical activity in obese adolescents: Effects of exercise training. Pediatr. Obes. 2016, 11, 26–32. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Delany, J.P.; Otto, A.D.; Kuller, L.; Vockley, J.; South-Paul, J.E.; Thomas, S.B.; Brown, J.; McTigue, K.; Hames, K.C.; et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: A randomized trial. JAMA 2010, 304, 1795–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.A.; Park, H.S. Relation between sleep duration, overweight, and metabolic syndrome in Korean adolescents. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 65–71. [Google Scholar] [CrossRef]
- Haseli-Mashhadi, N.; Dadd, T.; Pan, A.; Yu, Z.; Lin, X.; Franco, O.H. Sleep quality in middle-aged and elderly Chinese: Distribution, associated factors and associations with cardio-metabolic risk factors. BMC Public Health 2009, 9, 130. [Google Scholar] [CrossRef] [Green Version]
- Tan, X.; Alén, M.; Wiklund, P.; Partinen, M.; Cheng, S. Effects of aerobic exercise on home-based sleep among overweight and obese men with chronic insomnia symptoms: A randomized controlled trial. Sleep Med. 2016, 25, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Rognvaldsdottir, V.; Brychta, R.J.; Hrafnkelsdottir, S.M.; Chen, K.Y.; Arngrimsson, S.A.; Johannsson, E.; Guðmundsdottir, S.L. Less physical activity and more varied and disrupted sleep is associated with a less favorable metabolic profile in adolescents. PLoS ONE 2020, 15, e0229114. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, S.P.; Camps, S.G.; Gonnissen, H.K.; Westerterp, K.R.; Westerterp-Plantenga, M.S. Concomitant changes in sleep duration and body weight and body composition during weight loss and 3-mo weight maintenance. Am. J. Clin. Nutr. 2013, 98, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Jurado-Fasoli, L.; De-la-O, A.; Molina-Hidalgo, C.; Migueles, J.H.; Castillo, M.J.; Amaro-Gahete, F.J. Exercise training improves sleep quality: A randomized controlled trial. Eur. J. Clin. Investig. 2020, 50, e13202. [Google Scholar] [CrossRef] [PubMed]
- Knöpfli, B.H.; Radtke, T.; Lehmann, M.; Schätzle, B.; Eisenblätter, J.; Gachnang, A.; Wiederkehr, P.; Hammer, J.; Brooks-Wildhaber, J. Effects of a Multidisciplinary Inpatient Intervention on Body Composition, Aerobic Fitness, and Quality of Life in Severely Obese Girls and Boys. J. Adolesc. Health 2008, 42, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Hageman, P.A.; Mroz, J.E. Weight loss is associated with improved quality of life among rural women completers of a web-based lifestyle intervention. PLoS ONE 2019, 14, e0225446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, D.; Lou, P.; Wang, J.; Zhang, P.; Sun, J.; Chang, G.; Xu, C. Interaction of sleep quality and anxiety on quality of life in individuals with type 2 diabetes mellitus. Health Qual. Life Outcomes 2020, 18, 150. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Lubrano, C.; Gnessi, L.; Marocco, C.; Di Lazzaro, L.; Polidoro, G.; Luisi, F.; Merola, G.; Mariani, S.; Migliaccio, S.; et al. Reduced sleep duration affects body composition, dietary intake and quality of life in obese subjects. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2016, 21, 501–505. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RT | HIIT | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weeks | Intensity (%1RM) | Reps | Time (min) | Sets | Rest (min) | E N° | Intensity perception | Time (min) | Sets | Rest (min) | Duration (min) |
| 1–2 | 40 | 20–25 | 1 | 3 | 2.0 | 3 | 6–7 | 1 | 4 | 2.0 | 45 |
| 3–4 | 40–50 | 25–30 | 1 | 3 | 2.0 | 3 | 6–7 | 1 | 4 | 2.0 | 45 |
| 5–6 | 45–50 | 30 | 1 | 3 | 1.5 | 4 | 6–7 | 1 | 5 | 1.5 | 45 |
| 7–8 | 45–50 | 30–35 | 1 | 3 | 1.5 | 4 | 7–8 | 1 | 5 | 1.5 | 45 |
| 9–10 | 50–55 | 25–30 | 1 | 3 | 1.5 | 4 | 7–8 | 1 | 5 | 1.5 | 45 |
| 11–12 | 50–55 | 25–30 | 1 | 3 | 1.5 | 4 | 7–8 | 1 | 6 | 1.5 | 45 |
| 13–14 | 50–55 | 30 | 1 | 3 | 1.0 | 4 | 7–8 | 1 | 6 | 1.0 | 45 |
| 15–16 | 50–55 | 30–35 | 1 | 3 | 1.0 | 4 | 8 | 1 | 6 | 1.0 | 45 |
| 17–18 | 55 | 30–35 | 1 | 3 | 1.0 | 4 | 8 | 1 | 7 | 1.0 | 45 |
| 19–20 | 55–60 | 30–35 | 1 | 3 | 1.0 | 4 | 8–9 | 1 | 7 | 1.0 | 45 |
| Outcomes | Good Sleep Quality | Poor Sleep Quality | Good vs. Poor Sleep Quality (Baseline) | Good vs. Poor Sleep Quality (∆Pre–Post) | |
|---|---|---|---|---|---|
| n | 15 | 14 | |||
| Age (years) | 38.0 ± 12.2 | 40.7 ± 11.6 | |||
| Height (m) | 1.58 ± 0.07 | 1.59 ± 0.09 | |||
| Bedtime | 22:32 | 22:45 | |||
| Time to fall asleep (min) | 69.64 | 45.65 | |||
| Wake time | 07:50 | 07:28 | |||
| Body mass (kg) | Pre | 101.2 ± 19.5 | 116.8 ± 22.0 | p = 0.190 | p = 0.667 |
| Post | 99.4 ± 18.9 * | 114.6 ± 21.6 * | |||
| p | 0.045 | 0.018 | |||
| Δ | −1.7 | −2.21 | |||
| ES | 0.09 | 0.10 | |||
| BMI (kg/m2) | Pre | 40.1 ± 5.8 | 46.1 ± 7.0 | p = 0.019 # | p = 0.667 |
| Post | 39.4 ± 5.6 * | 45.2 ± 6.6 ** | |||
| p | 0.049 | 0.015 | |||
| Δ | −0.71 | −0.92 | |||
| ES | 0.12 | 0.13 | |||
| Body fat (%) | Pre | 46.2 ± 4.2 | 50.2 ± 4.5 | p = 0.019 # | p =0.332 |
| Post | 46.4 ± 4.0 | 49.9 ± 4.8 | |||
| p | 0.550 | 0.437 | |||
| Δ | 0.23 | −0.31 | |||
| ES | 0.06 | 0.07 | |||
| Body fat (kg) | Pre | 47.1 ± 11.5 | 59.4 ± 15.1 | p = 0.020 # | p = 0.306 |
| Post | 46.7 ± 11.4 | 58.0 ± 15.1 | |||
| p | 0.468 | 0.040 * | |||
| Δ | −0.45 | −1.38 | |||
| ES | 0.04 | 0.09 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delgado-Floody, P.; Latorre-Román, P.Á.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Cano-Montoya, J.; Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; Pozuelo-Carrascosa, D.P.; Álvarez, C. Poor Sleep Quality Decreases Concurrent Training Benefits in Markers of Metabolic Syndrome and Quality of Life of Morbidly Obese Patients. Int. J. Environ. Res. Public Health 2020, 17, 6804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186804
Delgado-Floody P, Latorre-Román PÁ, Jerez-Mayorga D, Caamaño-Navarrete F, Cano-Montoya J, Laredo-Aguilera JA, Carmona-Torres JM, Cobo-Cuenca AI, Pozuelo-Carrascosa DP, Álvarez C. Poor Sleep Quality Decreases Concurrent Training Benefits in Markers of Metabolic Syndrome and Quality of Life of Morbidly Obese Patients. International Journal of Environmental Research and Public Health. 2020; 17(18):6804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186804
Chicago/Turabian StyleDelgado-Floody, Pedro, Pedro Ángel Latorre-Román, Daniel Jerez-Mayorga, Felipe Caamaño-Navarrete, Johnattan Cano-Montoya, José Alberto Laredo-Aguilera, Juan Manuel Carmona-Torres, Ana Isabel Cobo-Cuenca, Diana P. Pozuelo-Carrascosa, and Cristian Álvarez. 2020. "Poor Sleep Quality Decreases Concurrent Training Benefits in Markers of Metabolic Syndrome and Quality of Life of Morbidly Obese Patients" International Journal of Environmental Research and Public Health 17, no. 18: 6804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186804